European Journal of Radiology Extra 51 (2004) 107–108
Inflamed pulmonary hamartoma Olga Rachel Brooka,∗ , Lael-Anson Bestb , Ludmila Guralnika a
Department of Diagnostic Imaging, Rambam Medical Center, POB 9602, Haifa 31096, Israel b Department of Thoracic Surgery, Rambam Medical Center, Haifa, Israel Received 25 March 2004; received in revised form 10 June 2004; accepted 16 June 2004
Abstract We present a case of pulmonary hamartoma with typical primary radiological findings, but with unusual radiological follow-up and abscess-like findings from CT guided fine needle aspiration. The final pathology report of the specimen confirmed the radiological diagnosis of pulmonary hamartoma. In retrospect, inflammation was radiologically indicated by a small amount of pleural effusion and diminishment of the lesion in a period of 1 month. © 2004 Elsevier Ireland Ltd. All rights reserved. Keywords: Biopsy; CT; Diagnosis; Hamartoma; Lung; Lung neoplasm
1. Introduction We report a case of pulmonary hamartoma with an unusual presentation of an inflammatory process, not yet described in the literature.
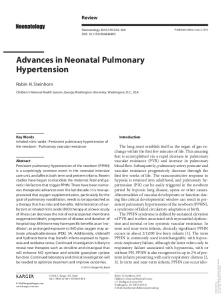
2. Case presentation A 47-year-old male with a history of arterial hypertension and non-insulin dependent diabetes mellitus presented with complaints of dry cough and left lower chest pain. He was treated with a full course of antibiotics with no change in symptoms for 2 months. CT examination (Fig. 1) showed a 3.8 cm × 3.1 cm lesion with typical characteristics of pulmonary hamartoma. The lesion was accompanied by a small amount of pleural effusion on the same side. Follow-up chest radiography (not shown) taken 1 month later for persistent cough revealed a substantial reduction in the size of the lesion, a feature not characteristic of pulmonary Abbreviations: CT, Computed tomography; FNA, Fine needle aspiration Corresponding author. Tel.: +97 24 8543682; fax: +97 24 8542690. E-mail address: o
[email protected] (O.R. Brook). ∗
1571-4675/$ – see front matter © 2004 Elsevier Ireland Ltd. All rights reserved. doi:10.1016/j.ejrex.2004.06.005
hamartoma. This necessitated further evaluation of the lesion. The patient underwent CT-guided FNA of the mass. The pre-FNA CT scan that was performed in prone position showed a marked reduction of the lesion to 2.4 cm × 2.3 cm (the slice with maximal size of the lesion); no pleural effusion was noted at this time (Fig. 2). The cytologist reported that the specimen contained numerous granulocytes, histiocytes, macrophages, respiratory epithelial cells, metaplastic cells and granulation tissue. It was concluded that these findings could be compatible with an abscess. Due to continuous complaints of dry cough, noncharacteristic behaviour of the lesion (that was initially thought as pulmonary hamartoma) and the result of FNA the patient were referred for wedge resection of the supposed abscess. The final pathology of the lung specimen was described as a 2.5 cm × 2.2 cm mass in close proximity to the pleura but without invasion. Macroscopically, it was grey hard tissue with little gelatinous material in it. Microscopically, it was pulmonary chondromatous hamartoma. The patient is now well, 4 months after the surgery.
108
O.R. Brook et al. / European Journal of Radiology Extra 51 (2004) 107–108
3. Discussion
Fig. 1. Initial contrast-enhanced axial CT scan (soft tissue window) at the level or right diaphragm. The 3.8 cm × 3.1 cm lesion with ‘popcorn’ calcifications is seen in the left lower lobe. A minimal amount of pleural effusion is also present.
Pulmonary hamartoma is a benign lung tumor whose clinical, radiological and pathological presentations are known [1–4]. Usually patients are asymptomatic, some may present with non-specific complaints. Abscess-like findings at FNA were not reported previously. Its clinical and radiological behaviour was also unusual and suited more the diagnosis of abscess—the lesion actually shrank in a period of 1 month and pleural effusion noted in a small amount on the first examination disappeared. This small amount of pleural fluid is likely the only radiological finding that could have directed us to the correct, although very unusual, diagnosis of inflamed hamartoma. Pulmonary parenchymal hamartoma contains mainly avascular cartilage. Still, it does contain some bronchial epithelium, which has a vascular supply and connection to some bronchi. Thus, it may get inflamed, as any other lung tissue, though this has not been reported in literature, as yet. We report the case where clinical and cytological findings of the pulmonary lesion suggested abscess, but radiological and pathological diagnosis gave final diagnosis of pulmonary hamartoma.
Acknowledgments The authors thank Prof. A. Rosenberger for thoughtful comments and Mrs. M. Perlmutter for her help in the preparation of this paper.
References
Fig. 2. Axial CT scan without contrast prior to the CT-guided FNA (soft tissue window) (the image was acquired in the prone position and then inverted) at the level of the diaphragm. The lesion has shrunk to 2.5 cm × 2.2 cm. No pleural effusion is seen now.
[1] Hansen CP, Holtveg H, Francis D, Rasch L, Bertelsen S. Pulmonary hamartoma. J Thorac Cardiovasc Surg 1992;104:674–8. [2] Fudge TL, Ochsner JL, Mills NL. Clinical spectrum of pulmonary hamartomas. Ann Thorac Surg 1980;30:36–9. [3] Poirier TJ, Van Ordstrand HS. Pulmonary chondromatous hamartomas: report of 17 cases and review of the literature. Chest 1971;59: 50–5. [4] Gjevre JA, Myers JL, Prakash UBS. Pulmonary hamartoma. Mayo Clin Proc 1996;71:14–20.