Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Young L, Embleton ND, McCormick FM, McGuire W
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2013, Issue 4 http://www.thecochranelibrary.com
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
TABLE OF CONTENTS HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Figure 1. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Figure 2. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Figure 3. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Figure 4. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Figure 5. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Figure 6. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Analysis 1.1. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 1 Weight (g). Analysis 1.2. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 2 Head circumference (cm). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Analysis 1.3. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 3 Length (cm). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Analysis 1.4. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 4 Visual acuity (cycles/degree). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Analysis 1.5. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 5 Contrast sensitivity (log). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Analysis 1.6. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 6 Bone mineral content (g). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Analysis 1.7. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 7 Bone mineral density (g/cm2 ). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Analysis 1.8. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 8 Duration of human milk feeding. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . Analysis 1.9. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 9 Proportion of infants fed with breast milk at end of intervention period. . . . . . . . . . . . . . . . . . . WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
1 1 2 2 3 3 5 6 7 7 8 8 9 9 11 11 11 13 17 18 19 20 21 21 22 22 23 23 23 24 24 25 25 25
i
[Intervention Review]
Multinutrient fortification of human breast milk for preterm infants following hospital discharge Lauren Young1 , Nicholas D Embleton2 , Felicia M McCormick3 , William McGuire1 1 Hull
York Medical School & Centre for Reviews and Dissemination, University of York, York, UK. 2 Newcastle Neonatal Service, Royal Victoria Infirmary, Newcastle upon Tyne, UK. 3 Mother and Infant Research Unit, Department of Health Sciences, University of York, York, UK Contact address: William McGuire, Hull York Medical School & Centre for Reviews and Dissemination, University of York, York, Y010 5DD, UK.
[email protected].
Editorial group: Cochrane Neonatal Group. Publication status and date: Edited (no change to conclusions), published in Issue 4, 2013. Review content assessed as up-to-date: 10 September 2012. Citation: Young L, Embleton ND, McCormick FM, McGuire W. Multinutrient fortification of human breast milk for preterm infants following hospital discharge. Cochrane Database of Systematic Reviews 2013, Issue 2. Art. No.: CD004866. DOI: 10.1002/14651858.CD004866.pub4. Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
ABSTRACT Background Preterm infants are usually growth restricted at hospital discharge. Feeding preterm infants after hospital discharge with multinutrient fortified breast milk rather than unfortified breast milk may facilitate more rapid catch-up growth and improve neurodevelopmental outcomes. Objectives To determine the effect of feeding preterm infants following hospital discharge with multinutrient fortified human breast milk versus unfortified breast milk on growth and development. Search methods We used the standard search strategy of the Cochrane Neonatal Review Group. This included electronic searches of the Cochrane Central Register of Controlled Trials Register (CENTRAL, The Cochrane Library, 2012, Issue 3), MEDLINE, EMBASE and CINAHL (until August 2012), conference proceedings, and previous reviews. Selection criteria Randomised or quasi-randomised controlled trials that compared feeding preterm infants following hospital discharge with multinutrient fortified breast milk compared with unfortified human breast milk. Data collection and analysis We extracted data using the standard methods of the Cochrane Neonatal Review Group with separate evaluation of trial quality and data extraction by two review authors and synthesis of data using risk ratio, risk difference and mean difference. Main results We identified two small trials involving a total of 246 infants. These did not provide evidence that multinutrient fortification of breast milk for three to four months after hospital discharge affected rates of growth during infancy. One trial assessed infants at 18 months corrected age and did not find any statistically significant effects on neurodevelopmental outcomes. Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
1
Authors’ conclusions The limited available data do not provide convincing evidence that feeding preterm infants with multinutrient fortified breast milk compared with unfortified breast milk following hospital discharge affects important outcomes including growth rates during infancy. There are no data on long-term growth. Since fortifying breast milk for infants fed directly from the breast is logistically difficult and has the potential to interfere with breast feeding, it is important to determine if mothers would support further trials of this intervention.
PLAIN LANGUAGE SUMMARY Multicomponent fortification of human breast milk for preterm infants following hospital discharge Preterm infants are often much smaller than term infants by the time that they are discharged home from hospital. This review appraised trials that evaluated whether feeding these infants with breast milk fortified with added nutrients rather than unfortified breast milk would increase growth rates and benefit development. We found only two small trials (involving 246 infants) of this intervention. These trials did not provide consistent evidence that multinutrient fortification affects growth rates during infancy. Further trials are needed to resolve this question and to assess long-term effects on growth and development.
BACKGROUND
Description of the condition Most preterm infants accumulate energy, protein, mineral, and other nutrient deficits by the time of discharge from hospital (Embleton 2001). At this stage, many preterm infants, especially those born with extremely low birth weight, are substantially growth restricted (Lucas 1984; Clark 2003). Following hospital discharge, demand-fed preterm infants consume greater volumes of milk than term infants of the same postmenstrual age in order to attain some “catch up” growth (Lucas 1992). Despite this, growth deficits can persist through infancy and beyond (Morley 2000; Ford 2000; Euser 2008). Slow postnatal growth in preterm infants is associated with neurodevelopmental impairment in later childhood and with poorer cognitive and educational outcomes (Hack 1991; Cooke 2003). Preterm infants who have accumulated deficits in calcium and phosphate by the time of hospital discharge have a higher risk of low bone mineralisation, metabolic bone disease, and slow skeletal growth compared with infants born at term (Rigo 2000). Furthermore, concern exists that nutritional deficiency and growth restriction in utero and during early infancy may have consequences for long-term metabolic and cardiovascular health (Barker 2002; Huxley 2002).
Description of the intervention Although human milk is the recommended nutritional source for newborn infants for at least the first six months of postnatal life
(WHO 2001), unfortified human breast milk may not meet the recommended nutritional needs of growing preterm infants (Tsang 1993; Greer 2007). Feeding preterm infants prior to hospital discharge with expressed human breast milk fortified with energy, protein, and minerals is associated with short-term increases in rates of weight gain and linear and head growth (Kuschel 2004a). Multinutrient breast milk fortifiers contain various amounts of protein, carbohydrate, minerals, and vitamins. These liquid or powder formulations are mixed with expressed breast milk for delivery with the aim of achieving about 5% to 10% nutrient enrichment (Simmer 2000). However, standard clinical practice has been to cease multinutrient fortification during the period prior to hospital discharge when breast feeding is being established since, following hospital discharge, human milk-fed preterm infants usually obtain most of their milk directly from the breast. It is feasible to continue nutritional supplementation for human milk-fed preterm infants in the post hospital discharge period of early infancy. Multinutrient fortification may be more practical for infants who are fed expressed breast milk (rather than directly from the breast) and may be especially important for infants who receive donated expressed breast milk which may contain lower levels of energy, protein and minerals than maternal expressed breast milk (Gross 1980). Mothers who feed their infants directly from the breast may also express breast milk and give at least some fortified feeds via a bottle, cup, or feeding tube. However, concern exists that this “medicalisation” of infant feeding might alter the maternal perception that breast milk is the preferred nutrition for her infant and interfere with the continuation of exclusive breast milk feeding.
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
2
Another putative disadvantage of multinutrient fortification of breast milk is that increasing the nutrient density and osmolarity of breast milk might interfere with gastric emptying and intestinal peristalsis, resulting in feed intolerance, vomiting or diarrhoea. Observational studies have provided conflicting evidence on these potential adverse effects (Ewer 1996; McClure 1996). The Cochrane review of multinutrient fortification of human milk for preterm infants prior to hospital discharge did not find any evidence of a higher incidence of gastrointestinal adverse effects in infants who received fortified milk (Kuschel 2004a). There is also concern that excessive protein supplementation may cause metabolic stresses resulting in acidosis or elevated blood urea levels. However, the Cochrane reviews of multinutrient fortification and of protein supplementation of human milk for preterm infants prior to hospital discharge did not find evidence that blood urea rose to levels outwith normal reference ranges (Kuschel 2004a; Kuschel 2004b). Finally, concern exists that rapid catch-up growth during early infancy may have metabolic programming effects that increase the long-term risk of overweight and obesity, insulin resistance, diabetes, hypertension, and cardiovascular and cerebrovascular disease (Singhal 2003; Singhal 2004; Singhal 2007).
Uncertainty exists about the balance between the putative benefits and harms of multinutrient fortification of breast milk for preterm infants following hospital discharge. Since this intervention has the potential to affect several major outcomes, an attempt to detect, appraise, and synthesise evidence from randomised controlled trials is needed.
How the intervention might work
Types of studies
In theory, feeding preterm infants following hospital discharge with milk enriched with extra energy, protein, minerals and vitamins may be expected to promote more rapid catch-up growth. Higher levels of nutritional input during this period may be especially important for infants who are not able to consume ad libitum quantities of milk directly from the breast, who have slow growth, or who have on-going additional nutritional and metabolic requirements, for example, due to chronic lung disease (Cooke 2000; Griffin 2002; McLeod 2011). However, if preterm infants are fed in response to hunger and satiation cues (ad libitum or demand), they may adjust their volume of intake depending upon the energy-density of the milk and so consume less nutrient-fortified milk than if fed with unfortified breast milk. Consequently, infants fed ad libitum with nutrient-fortified milk may not receive any more nutrients than infants who receive unfortified breast milk. Furthermore, concern exists that catch-up growth with accelerated weight gain and crossing of body mass index (BMI) percentiles might be associated with altered fat distribution and related ‘programmed’ metabolic consequences that may increase the risk of insulin resistance and cardiovascular disease (Euser 2005; Euser 2008). However, any effects of nutritional interventions in early infancy on long-term health consequences are likely to be much smaller than those of other environmental or genetic factors (Greer 2007).
Why it is important to do this review
OBJECTIVES To determine the effect of feeding with multinutrient fortified human breast milk versus unfortified breast milk on growth and development in preterm infants following hospital discharge.
METHODS
Criteria for considering studies for this review
Controlled trials using random or quasi-random patient allocation. Studies published only as abstracts were eligible for inclusion provided assessment of study quality was possible and other criteria for inclusion fulfilled.
Types of participants Preterm infants (< 37 weeks’ gestation at birth) and low birth weight infants (< 2.5 kg) receiving human breast milk following discharge from hospital.
Types of interventions
Multinutrient fortification Supplementation of human breast milk with more than one nutrient (protein, fat, carbohydrate, or minerals [calcium and/or phosphate]), versus feeding with unsupplemented human milk. Supplementation with electrolytes, iron, vitamins, or trace minerals in addition to only one of the above nutrients was not classified as multinutrient fortification for the purposes of this review. Restrictions to the pre-discharge feeding regimens were not prespecified. The intervention could have begun up to one week prior to planned discharge from hospital. Trials that randomly assigned infants to begin the study feed more than one week prior to hospital discharge (and then continued the intervention after hospital discharge) were not included in this review. Eligible studies should
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
3
have planned to allocate the trial intervention for a sufficient period (at least two weeks) to allow measurable effects on growth. Infants in the comparison groups within each study should have received similar care other than the level of fortification of breast milk. For example, there should not be any within-study differences in the prescription of target levels of volume of intake, or advice or support for demand feeding.
Types of outcome measures
Primary outcomes
1. Growth: Weight, length, head growth, skinfold thickness, BMI and measures of body composition (lean/fat mass) and growth-restriction (proportion of infants who remain < 10th percentile for the index population’s distribution of weight, length, or head circumference). 2. Development: (a) Neurodevelopmental outcomes assessed using validated tools at >12 months corrected age, and classifications of disability, including non-ambulant cerebral palsy, developmental delay, auditory and visual impairment, (b) Cognitive and educational outcomes at > five years: Intelligence quotient and/or indices of educational achievement measured using a validated tool (including school examination results).
Secondary outcomes
1. Feed intolerance defined as vomiting or diarrhoea that results in the infant requiring treatment for dehydration (for example, oral rehydration solution, or hospital admission, or intravenous rehydration). 2. Duration of breast milk-feeding (until infant stops receiving any human breast milk) and proportion of infants receiving any breast milk at end of intervention period. 3. Measures of bone mineralisation such as serum alkaline phosphatase level, or bone mineral content assessed by dual energy X-ray absorptiometry and clinical or radiological evidence of rickets on long-term follow-up. 4. Clinical or radiological evidence of rickets on long-term follow-up. 5. Blood pressure on long-term follow-up.
Search methods for identification of studies We used the standard search strategy of the Cochrane Neonatal Review Group. Electronic searches We searched the Cochrane Central Register of Controlled Trials (CENTRAL, The Cochrane Library, 2012, Issue 3), MEDLINE
(1966 to August 2012), EMBASE (1980 to August 2012), and CINAHL (1982 to August 2012) using a combination of the following text words and MeSH terms: [Infant, Newborn OR Infant, Premature OR Infant, Low Birth Weight OR infan* OR neonat*] AND [“Infant-Nutrition”/ all subheadings OR Milk, Human OR milk OR breast OR Infant Formula OR formula OR post-discharge OR fortif* OR supplement*]. The search outputs were limited with the relevant search filters for clinical trials as recommended in the Cochrane Handbook for Systematic Reviews of Interventions . We did not apply any language restrictions. We searched ClinicalTrials.gov and Current Controlled Trials for completed or ongoing trials. Searching other resources We examined the references in studies identified as potentially relevant. We also searched the abstracts from the annual meetings of the Pediatric Academic Societies (1993 to 2012), the European Society for Pediatric Research (1995 to 2011), the UK Royal College of Paediatrics and Child Health (2000 to 2012), and the Perinatal Society of Australia and New Zealand (2000 to 2012). We considered trials reported only as abstracts to be eligible if sufficient information was available from the report, or from contact with the authors, to fulfil the inclusion criteria.
Data collection and analysis We used the standard search strategy of the Cochrane Neonatal Review Group. Selection of studies Two review authors screened the title and abstract of all studies identified by the above search strategy. We reassessed the full text of any potentially eligible reports and excluded those studies that did not meet all of the inclusion criteria. We discussed any disagreements until consensus was achieved. Data extraction and management We used a data collection form to aid extraction of relevant information from each included study. Two review authors extracted the data separately. We discussed any disagreements until consensus was achieved. We asked the investigators for further information if data from the trial reports were insufficient.
Assessment of risk of bias in included studies We used the criteria and standard methods of the Cochrane Neonatal Review Group to assess the methodological quality of any included trials. Additional information from the trial authors was requested to clarify methodology and results as necessary. We
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
4
evaluated and reported the following issues in the ’Risk of bias’ tables: 1. Sequence generation: We categorised the method used to generate the allocation sequence as: i) low risk: any random process e.g. random number table; computer random number generator; ii) high risk: any non random process e.g. odd or even date of birth; patient case-record number); iii) unclear. 2. Allocation concealment: We categorised the method used to conceal the allocation sequence as: i) low risk: e.g. telephone or central randomisation; consecutively numbered sealed opaque envelopes; ii) high risk: open random allocation; unsealed or nonopaque envelopes, alternation; date of birth; iii) unclear. 3. Blinding: We assessed blinding of participants, clinicians and caregivers, and outcome assessors separately for different outcomes and categorised the methods as: i) low risk; ii) high risk; iii) unclear. 4. Incomplete outcome data: We described the completeness of data including attrition and exclusions from the analysis for each outcome and any reasons for attrition or exclusion where reported. We assessed whether missing data were balanced across groups or were related to outcomes. Where sufficient information was reported or supplied by the trial authors, we re-included missing data in the analyses. We categorised completeness as: i) low risk: < 20% missing data; ii) high risk: > 20% missing data; iii) unclear.
We calculated the I² statistic for each analysis to quantify inconsistency across studies and describe the percentage of variability in effect estimates that may be due to heterogeneity rather than sampling error. If substantial (I² > 50%) heterogeneity was detected, we explored the possible causes (for example, differences in study design, participants, interventions, or completeness of outcome assessments) in sensitivity analyses. Assessment of reporting biases If more than five trials had been included in a meta-analysis, we planned to conduct a funnel plot analysis. Subgroup analysis and investigation of heterogeneity We pre-specified the following subgroup analyses: 1. very preterm (< 32 weeks) or very low birth weight (VLBW) (< 1500 g) infants; 2. infants who were small for gestational age (< 10th percentile for the index population’s distribution of weight) at hospital discharge; 3. infants with chronic lung disease receiving supplemental oxygen therapy at hospital discharge; 4. infants who receive donated expressed breast milk.
RESULTS
Description of studies See: Characteristics of included studies; Characteristics of excluded studies.
Measures of treatment effect We calculated risk ratio (RR) and risk difference (RD) for dichotomous data and mean difference (MD) for continuous data, with respective 95% confidence intervals (CI). We calculated the number needed to treat for benefit (NNTB) or harm (NNTH) for a statistically significant difference in the RD.
Unit of analysis issues The unit of analysis is the participating infant in individuallyrandomised trials and the neonatal unit (or sub-unit) for clusterrandomised trials.
Assessment of heterogeneity If more than one trial had been included in a meta-analysis, we planned to examine the treatment effects of individual trials and heterogeneity between trial results by inspecting the forest plots.
Included studies We identified two eligible trials involving 246 infants (see ’Characteristics of included studies’ table). • O’Connor 2008: The investigators randomly allocated 39 breast milk-fed preterm infants (< 33 weeks’ gestation at birth) who were due to be discharged from hospital to receive multinutrient fortifier mixed with expressed breast milk (about half of their estimated total daily milk intake) or to continue with unfortified human milk feeding for 12 weeks postdischarge. The investigators anticipated that, at discharge, infants in the intervention group would receive about 10% more energy and 20% more protein than the controls. Outcomes assessed were growth and bone mineral content and density up to 12 months corrected age, duration of breast feeding, visual acuity and contrast sensitivity at four and six months corrected age, and Bayley II mental development index (MDI) and psychomotor development index (PDI) scores at 18 months corrected age.
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
5
• Zachariassen 2011: The investigators randomly allocated 207 breast feeding preterm infants (< 33 weeks’ gestation at birth) “shortly before” hospital discharge to receive multinutrient fortifier (total energy content 17.5 kCal, protein 1.375 g) mixed with 20 mL to 50 mL of expressed breast milk once daily or to continue with unfortified human milk feeding until four months post term. This level of supplementation (for an infant weighing 2.2 kg receiving 180 mL/kg/day) equates to about 6.5% more energy and 20% more protein than controls. Outcomes assessed were growth parameters up to 12 months corrected age and duration of breast feeding. Excluded studies We excluded one trial as the intervention group received only mineral fortification (Hall 1993; see ’Characteristics of excluded studies’ table).
Risk of bias in included studies In both trials, allocation generation and concealment were adequate. Blinding of the intervention was not attempted but blinding of some assessments (including developmental assessment) was
possible. Both trials achieved near complete follow-up assessment at the end of the intervention period and reported intention-totreat outcome data (see ’Characteristics of included studies’ table).
Effects of interventions
PRIMARY OUTCOMES
Growth (Outcomes 1.1 to 1.3) Meta-analyses of data from both trials did not find statistically significant differences in growth parameters at three to four months corrected age. Meta-analyses did not find statistically significant differences in weight or head circumference at 12 months corrected age but infants in the intervention group were borderline statistically significantly longer than control infants; MD 0.88 (95% CI 0.01 to 1.74 cm). All of the meta-analyses contained statistically significant heterogeneity, in each case O’Connor 2008 found a larger (and statistically significant) mean difference than Zachariassen 2011 (Figure 1; Figure 2; Figure 3).
Figure 1. Forest plot of comparison: 1 Multinutrient fortification vs. no fortification of human breast milk, outcome: 1.1 Weight (g).
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
6
Figure 2. Forest plot of comparison: 1 Multinutrient fortification vs. no fortification of human breast milk, outcome: 1.2 Head circumference (cm).
Figure 3. Forest plot of comparison: 1 Multinutrient fortification vs. no fortification of human breast milk, outcome: 1.3 Length (cm).
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
7
Neurodevelopmental outcomes (Outcomes 1.4 to 1.5) O’Connor 2008 did not detect any statistically significant differences in Bayley II MDI and PDI scores at 18 months corrected age (27 infants assessed). • MDI: 100 (1st to 3rd centile; 72 to 102.5) versus 91 (1st to 3rd centile; 77 to 107). • PDI: 94 (1st to 3rd centile; 90 to 99) versus 94 (1st to 3rd centile; 86 to 103). O’Connor 2008 reported that visual acuity assessed using sweep visual-evoked potential testing at four months and at six months was statistically significantly higher in the intervention group (Figure 4).The same assessments did not detect statistically significant differences in contract sensitivity (Figure 5). Figure 4. Forest plot of comparison: 1 Multinutrient fortification vs. no fortification of human breast milk, outcome: 1.4 Visual acuity (cycles/degree).
Figure 5. Forest plot of comparison: 1 Multinutrient fortification vs. no fortification of human breast milk, outcome: 1.5 Contrast sensitivity (log).
Cognitive and educational outcomes:
Not reported by either trial.
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
8
SECONDARY OUTCOMES
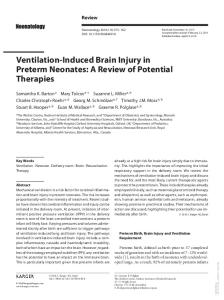
Bone mineralisation (Outcomes 1.6) O’Connor 2008 reported that bone mineral content was statistically significantly higher in the intervention group at four months (mean difference (MD) 20.60 (95% confidence interval (CI) 6.41 to 34.79 g)) and 12 months (MD 29.80 (95% CI 3.63 to 55.97 g)) (Figure 6). Bone mineral density was not statistically significantly different. Figure 6. Forest plot of comparison: 1 Multinutrient fortification vs. no fortification of human breast milk, outcome: 1.6 Bone mineral content (g).
Feed intolerance Not reported by either trial.
Blood pressure on long-term follow-up Not reported by either trial.
Subgroup analyses Breast milk feeding (Outcomes 1.8 to 1.9) Neither trial found a statistically significant difference in the duration of breast milk feeding. Meta-analysis was not appropriate since O’Connor 2008 reported this outcome as “post natal weeks” and Zachariassen 2011 reported “post term weeks”. Zachariassen 2011 reported that statistically significantly fewer infants in the intervention group remained exclusively fed with human milk (no formula) at four months: risk ratio (RR) 0.48 (95% CI 0.30 to 0.76) (Analysis 1.9) (proportion still at least partially fed not reported). O’Connor 2008 did not find a statistically significant difference in the proportion of infants receiving any breast milk at the end of the intervention period.
Data were not available for any of the prespecified analyses: 1. very low birth weight or very preterm infants: In both trials participants were of gestational age < 33 weeks at birth; 2. infants who were small for gestational age at hospital discharge: In O’Connor 2008, three of 39 participants were small for gestational age. In Zachariassen 2011 41 of 207 participants were small for gestational age. Subgroup outcome data were not available; 3. infants with chronic lung disease requiring home supplemental oxygen therapy: None of the participants received home supplemental oxygen therapy; 4. infants who received donated expressed breast milk: none of the participants received donated expressed breast milk.
Clinical or radiological evidence of rickets on long-term follow-up Not reported by either trial.
DISCUSSION
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
9
Summary of main results Two small randomised controlled trials involving 246 infants did not provide consistent evidence that feeding preterm infants with multinutrient fortified versus unfortified human breast milk for three to four months post-discharge affects growth parameters through infancy (O’Connor 2008; Zachariassen 2011). The identified trials reported very limited data on developmental outcomes and have not yet assessed any longer-term growth or health outcomes.
Overall completeness and applicability of evidence The meta-analyses of growth outcomes contained substantial statistical heterogeneity and need to be interpreted cautiously. In each case O’Connor 2008 found a larger (and statistically significant) mean difference than Zachariassen 2011. The participants in the trials were similar (< 33 weeks gestation at birth, breast-fed at discharge). The overall target level of multinutrient fortification was also similar. Both trials intended to provide extra energy, protein and minerals such that infants received total levels of nutrient input comparable to infants receiving commercially-available “postdischarge formula” (72 kCal to 74 kCal and about 1.6 to 1.8 g of protein/100 mL, plus proportionate supplements of minerals, vitamins, and trace elements). The trials differed slightly in the mechanics of delivering the multinutrient fortifier. In O’Connor 2008, infants received fortifier in about half of their daily intake of breast milk whereas in Zachariassen 2011 the fortifier was given once daily mixed in 20 mL to 50 mL of milk. In both trials the remaining feeds were either taken directly from the breast or as unfortified expressed breast milk ad libitum. It is unclear whether the slightly different methods of providing fortifier had different impacts on the infants’ responses to the energy density of their feeds, in particular whether infants titrated overall volume of intake differently depending on whether they received fortifier in half their feeds or in a once daily feed. Zachariassen 2011 did not report any data on overall levels of nutrient intake in trial participants. However, O’Connor 2008 reported that the estimated total volume of milk consumed differed between the groups. At the end of the 12 weeks intervention period, infants in the intervention group consumed a mean daily volume of 111 mL/kg compared with 134 mL/kg in the control group. Consequently, the intervention group did not receive substantially different amounts of energy (79 versus 87 kCal/kg/day in the control group) or protein (1.9 versus 1.7 g/kg/day). However, infants in the intervention group received statistically significantly more calcium (11.9 versus 4.7 mmol/kg/day) and phosphorous (8.7 versus 3.8 mmol/kg/day) than control infants. Similarly, intake of vitamin D was higher in the intervention group (567 versus 380 IU/kg/day at 12 weeks). These differences in mineral and vitamin D intake in O’Connor
2008 are possible explanations for the detection of higher whole body bone mineral content in the intervention group maintained until 12 months post term. Bone density and estimated total and percentage fat mass at 12 months were not statistically significantly different suggesting that a higher rate of skeletal growth may be the most important cause of the differences in weight, length and head circumference between the groups. These findings are consistent with data from observational studies that compared preterm infants fed with unfortified breast milk versus formula milk following hospital discharge. These studies found higher levels of bone mineralisation in the formula-fed group suggesting that breast milk mineral or vitamin content may be rate limiting with regard to skeletal growth during early infancy (Chan 1985; Abrams 1988).
Quality of the evidence Although small, the trials were generally of good methodological quality with adequate measures to conceal random allocation and near-complete follow-up assessment during the intervention period. Blinding of parents and caregivers was not possible given the nature of the intervention. This is not likely to be a source of bias in growth assessments. However, knowledge of the intervention group may have affected caregivers’ or mothers’ perceptions and views of feeding and may have influenced decisions on whether to give any formula as a supplement to (or instead of ) breast feeding. The trials did not find evidence that multinutrient fortification affected the duration of breast feeding. O’Connor 2008 did not find a difference in the proportion of infants receiving any breast milk at the end of the intervention period. In part, this finding may be due to the provision of intensive lactation support from the study co-ordinator for both groups during the trial period. Whether breast feeding rates can be maintained in the absence of intensive support remains to be determined. Zachariassen 2011 did not report he proportion of infants receiving any breast milk at the end of the intervention period. However, this trial did detect a statistically significant reduction in the proportion of intervention group infants receiving exclusive breast milk feeding at four months post term.
Agreements and disagreements with other studies or reviews The Cochrane review of trials of nutrient-enriched formula versus standard term formula (which contains about the same level of energy, protein and other nutrients as human breast milk) for feeding preterm infants following hospital discharge did not find an effect on growth rates during infancy (Young 2012). This review also found evidence that infants fed ad libitum infants reduce their volume of intake when the energy content of the milk is higher. Consequently, infants fed ad libitum with nutrient-enriched formula
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
10
milk generally receive similar levels of calories and only slightly more protein and minerals than infants who receive standard term formula. Therefore, the lack of an effect on growth may be due to the differential in bone mineral or vitamin levels of intake being less marked than in the comparison of multinutrient fortified and unfortified breast milk. Given these findings, it is important that future studies attempt to determine whether bone mineral (and/ or vitamin D) supplementation has a similar effect on catch-up growth rates as multinutrient fortification (Hall 1993).
AUTHORS’ CONCLUSIONS
Implications for research Given the potential for post-discharge nutrient fortification of breast milk to affect growth and development in preterm infants, this intervention merits further assessment. Further work is also needed to determine which nutrient groups confer the most important benefits to growth and development. Since fortifying breast milk for infants fed directly from the breast is logistically difficult (and has the potential to interfere with breast feeding), it is important to determine if mothers would support a trial of this intervention. It may be that a trial should first focus on infants who are not able to consume ad libitum quantities of milk directly from the breast, who have low rates of in hospital growth, or who have on-going additional metabolic requirements, for example, due to chronic lung disease.
Implications for practice The limited available data do not provide evidence that feeding preterm infants following hospital discharge with multinutrient fortified breast milk compared with unfortified breast milk affects growth rates during infancy. The effect on long-term growth and development has not been assessed.
ACKNOWLEDGEMENTS We thanks Drs Deborah O’Connor and Dr Gitte Zachariassen for providing further information regarding their trials (O’Connor 2008; Zachariassen 2011
REFERENCES
References to studies included in this review O’Connor 2008 {published data only} Aimone A, Rovet J, Ward W, Jefferies A, Campbell DM, Asztalos E, et al.Growth and body composition of human milk-fed premature infants provided with extra energy and nutrients early after hospital discharge: 1-year follow-up. Journal of Pediatric Gastroenterology and Nutrition 2009;49 (4):456–66. O’Connor DL, Khan S, Weishuhn K, Vaughan J, Jefferies A, Campbell DM, et al.Growth and nutrient intakes of human milk-fed premature infants provided with extra energy and nutrients after hospital discharge. E-PAS:60: 7720.6. Pediatric Academic Societies’s Annual Meeting, 2007. ∗ O’Connor DL, Khan S, Weishuhn K, Vaughan J, Jefferies A, Campbell DM, et al.Growth and nutrient intakes of human milk-fed preterm infants provided with extra energy and nutrients after hospital discharge. Pediatrics 2008;121 (4):766–76. O’Connor DL, Weishuhn K, Rovet J, Mirabella G, Jefferies A, Campbell DM, et al.Visual development of human milkfed preterm infants provided with extra energy and nutrients after hospital discharge. Journal of Parenteral and Enteral Nutrition 2012;36(3):349–53. Zachariassen 2011 {published data only} Zachariassen G, Faerk J, Esberg BH, Fenger-Gron J, Mortensen S, Christesen HT, et al.Allergic diseases among very preterm infants according to nutrition after hospital
discharge. Pediatric Allergy and Immunology 2011;22(5): 515–20. [PUBMED: 21332800] ∗ Zachariassen G, Faerk J, Grytter C, Esberg BH, Hjelmborg J, Mortensen S, et al.Nutrient enrichment of mother’s milk and growth of very preterm infants after hospital discharge. Pediatrics 2011;127(4):e995–e1003. [PUBMED: 21402642]
References to studies excluded from this review Hall 1993 {published data only} Hall RT, Wheeler RE, Rippetoe LE. Calcium and phosphorus supplementation after initial hospital discharge in breast-fed infants of less than 1800 grams birth weight. Journal of Perinatology 1993;13(4):272–8.
Additional references Abrams 1988 Abrams SA, Schanler RJ, Garza C. Bone mineralization in former very low birth weight infants fed either human milk or commercial formula. The Journal of Pediatrics 1988;112 (6):956–60. Barker 2002 Barker DJ. Fetal programming of coronary heart disease. Trends in Endocrinology and Metabolism 2002;13(9):364–8. Chan 1985 Chan GM, Mileur LJ. Posthospitalization growth and bone mineral status of normal preterm infants. Feeding with
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
11
mother’s milk or standard formula. American Journal of Diseases of Children 1985;139(9):896–8. Clark 2003 Clark RH, Thomas P, Peabody J. Extrauterine growth restriction remains a serious problem in prematurely born neonates. Pediatrics 2003;111(5 Pt 1):986–90. Cooke 2000 Cooke RJ, Embleton ND. Feeding issues in preterm infants. Archives of Disease in Childhood. Fetal and Neonatal Edition 2000;83(3):F215–8. Cooke 2003 Cooke RWI, Foulder-Hughes L. Growth impairment in the very preterm and cognitive and motor performance at 7 years. Archives of Disease in Childhood 2003;88(6):482–7. Embleton 2001 Embleton NE, Pang N, Cooke RJ. Postnatal malnutrition and growth retardation: an inevitable consequence of current recommendations in preterm infants?. Pediatrics 2001;107(2):270–3. Euser 2005 Euser AM, Finken MJ, Keijzer-Veen MG, Hille ET, Wit JM, Dekker FW. Associations between prenatal and infancy weight gain and BMI, fat mass, and fat distribution in young adulthood: a prospective cohort study in males and females born very preterm. The American Journal of Clinical Nutrition 2005;81(2):480–7. [PUBMED: 15699238] Euser 2008 Euser AM, de Wit CC, Finken MJ, Rijken M, Wit JM. Growth of preterm born children. Hormone Research 2008; 70(6):319–28. Ewer 1996 Ewer AK, Yu VY. Gastric emptying in pre-term infants: the effect of breast milk fortifier. Acta Paediatrica 1996;85(9): 1112–5. Ford 2000 Ford GW, Doyle LW, Davis NM, Callanan C. Very low birth weight and growth into adolescence. Archives of Pediatrics & Adolescent Medicine 2000;154(8):778–84. Greer 2007 Greer FR. Post-discharge nutrition: what does the evidence support?. Seminars in Perinatology 2007;31(2):89–95.
Huxley 2002 Huxley R, Neil A, Collins R. Unravelling the fetal origins hypothesis: is there really an inverse association between birthweight and subsequent blood pressure?. Lancet 2002; 360(9334):659–65. Kuschel 2004a Kuschel CA, Harding JE. Multicomponent fortified human milk for promoting growth in preterm infants. Cochrane Database of Systematic Reviews 2004, Issue 1. [DOI: 10.1002/14651858.CD000343.pub2] Kuschel 2004b Kuschel CA, Harding JE. Protein supplementation of human milk for promoting growth in preterm infants. Cochrane Database of Systematic Reviews 2004, Issue 1. [DOI: 10.1002/14651858.CD000433] Lucas 1984 Lucas A, Gore SM, Cole TJ, Bamford MF, Dossetor JF, Barr I, et al.Multicentre trial on feeding low birthweight infants: effects of diet on early growth. Archives of Disease in Childhood 1984;59(8):722–30. Lucas 1992 Lucas A, King F, Bishop NB. Postdischarge formula consumption in infants born preterm. Archives of Disease in Childhood 1992;67(6):691–2. McClure 1996 McClure RJ, Newell SJ. Effect of fortifying breast milk on gastric emptying. Archives of Disease in Childhood. Fetal and Neonatal Edition 1996;74(1):F60–2. McLeod 2011 McLeod G, Simmer K, Benninger H, Mitoulas L, Doherty D, Sherriff J. Preterm infants with chronic lung disease: are protein and energy intakes after discharge sufficient for optimal growth?. Journal of Paediatrics and Child Health 2011;47(3):127–33. [PUBMED: 21091585] Morley 2000 Morley R, Lucas A. Randomized diet in the neonatal period and growth performance until 7.5-8 y of age in preterm children. American Journal of Clinical Nutrition 2000;71 (3):822–8.
Griffin 2002 Griffin IJ. Post discharge nutrition for high risk neonates. Clinics in Perinatology 2002;29(2):327–44.
Rigo 2000 Rigo J, De Curtis M, Pieltain C, Picaud JC, Salle BL, Senterre J. Bone mineral metabolism in the micropremie. Clinics in Perinatology 2000;27(1):147–70.
Gross 1980 Gross SJ, David RJ, Bauman L, Tomarelli RM. Nutritional composition of milk produced by mothers delivering preterm. Journal of Pediatrics 1980;96(4):641–4.
Simmer 2000 Simmer K. Choice of formula and human milk supplement for preterm infants in Australia. Journal of Paediatrics and Child Health 2000;36(6):593–5.
Hack 1991 Hack M, Breslau N, Weissman B, Aram D, Klein N, Borawski E. Effect of very low birthweight and subnormal head size on cognitive abilities at school age. New England Journal of Medicine 1991;325(4):231-7.
Singhal 2003 Singhal A, Fewtrell M, Cole TJ, Lucas A. Low nutrient intake and early growth for later insulin resistance in adolescents born preterm. Lancet 2003;361(9363): 1089–97.
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
12
Singhal 2004 Singhal A, Cole TJ, Fewtrell M, Deanfield J, Lucas A. Is slower early growth beneficial for long-term cardiovascular health?. Circulation 2004;109(9):1108–13.
Nutrient-enriched formula versus standard term formula for preterm infants following hospital discharge. Cochrane Database of Systematic Reviews 2012, Issue 3. [DOI: 10.1002/14651858.CD004696.pub4]
Singhal 2007 Singhal A, Cole TJ, Fewtrell M, Kennedy K, Stephenson T, Elias-Jones A, et al.Promotion of faster weight gain in infants born small for gestational age: is there an adverse effect on later blood pressure?. Circulation 2007;115(2): 213–20.
References to other published versions of this review
Tsang 1993 Tsang RC, Lucas A, Uauy R, Zlotkin S. Nutritional Needs of the Preterm Infant. Scientific Basis and Practical Guidelines. New York: Williams and Wilkins, 1993. WHO 2001 The World Health Organization. 54th World Health Assembly. 2001; Vol. 54.2. Young 2012 Young L, Morgan J, McCormick FM, McGuire W.
Henderson 2007 Henderson G, Fahey T, McGuire W. Multicomponent fortification of human breast milk for preterm infants following hospital discharge. Cochrane Database of Systematic Reviews 2007, Issue 4. [DOI: 10.1002/ 14651858.CD004866.pub2] McCormick 2010 McCormick FM, Henderson G, Fahey T, McGuire W. Multinutrient fortification of human breast milk for preterm infants following hospital discharge. Cochrane Database of Systematic Reviews 2010, Issue 7. [DOI: 10.1002/ 14651858.CD004866.pub3] ∗ Indicates the major publication for the study
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
13
CHARACTERISTICS OF STUDIES
Characteristics of included studies [ordered by study ID] O’Connor 2008 Methods
Randomised controlled trial
Participants
39 preterm infants born < 33 weeks’ gestation with birthweight 750-1800 g Enrolled when receiving 80% of enteral feedings orally as human milk (fortified or unfortified) 3 days before planned hospital discharge Exclusion criteria: infants with serious anomalies affecting growth; grade 3 or 4 periventricular haemorrhage; receipt of oral steroids within 14 days of randomisation; Apgar score < 5 at 5 minutes; known maternal alcohol or drug abuse; family habitat outside study area; mother unable to communicate verbally in English; infant needed nutrient enrichment incompatible with the intervention
Interventions
Intervention (N = 19): feeding after hospital discharge with human milk, half of which to be fortified with 3.6 g commercially-available powdered multinutrient human milk fortifier per 100 mL fresh or thawed human milk for 12 weeks following discharge Control (N = 20): “Standard care” - feeding after hospital discharge with unfortified human milk Both groups received standard vitamins and iron supplements post-discharge Both groups had access to intensive lactation support from the study co-ordinator, a certified lactation consultant, who also performed the study measures during home visits
Outcomes
1. Growth: weight , length and head circumference up to completion of intervention period (12 weeks post-discharge) and up to 12 months corrected age 2. Bayley II mental and psychomotor development index scores at 18 months corrected age 3. Bone mineral content and density at 4 months and 12 months corrected age 4. Nutrient intake up to completion of intervention period 5. Duration of breast milk feeding (at least one human milk feed per day) and proportion of daily feeds provided as human milk up to 12 weeks 6. Visual development: Grating acuity (i.e., visual acuity) and contrast sensitivity were assessed using sweep visual-evoked potential tests at 4 and 6 months corrected age
Notes
Aim with fortification of half of the daily human milk intake was to provide milk with an overall average calorie content of 74 kcal/100 mL and protein content of 1.8 g/100 mL; that is, about the same nutrient density as commercially-available “post-discharge” formula Infants in the intervention group did receive about 50% fortified feeds as planned. Infants in the control group received about 8% fortified feeds at each data collection point The investigators estimated that “energy intakes did not differ between the groups, suggesting human milk-fed infants are able to compensate to some degree for the energy and/or nutrient density of their feeding.” The authors acknowledge that the human milk fortifier and disposable supplies to collect and store human milk, were donated by Abbott Nutrition and Mead Johnson Nutritionals
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
14
O’Connor 2008
(Continued)
Risk of bias Bias
Authors’ judgement
Support for judgement
Random sequence generation (selection Low risk bias)
Computer-generated
Allocation concealment (selection bias)
Sequence stored in sealed envelopes
Low risk
Blinding (performance bias and detection High risk bias) All outcomes
Parents or other caregivers were not blind to intervention Unclear whether assessors (e.g. developmental assessment) were aware of intervention group
Incomplete outcome data (attrition bias) All outcomes
Outcome data not reported for five infants withdrawn post-randomisation (from total N = 39)
High risk
Zachariassen 2011 Methods
Randomised controlled trial
Participants
207 preterm infants born < 33 weeks’ gestation Enrolled ’shortly’ before planned hospital discharge Exclusion criteria: infants with serious diseases or circumstances influencing feeding ability at discharge
Interventions
Intervention (N = 105): once daily addition of a commercially available breast-milk fortifier containing 17.5 kCal and 1.375 g of protein to 20-50 mL of expressed breast milk. The fortified milk was fed via bottle or cup. The intervention was planned to continue until 4 months post term Control (N = 102): breast feeding after hospital discharge with unfortified human milk Use of vitamins or iron not described, level of lactation support not described
Outcomes
1. Growth: weight , length and head circumference up to 12 months corrected age 2. Duration of breast milk feeding (at least one human milk feed per day) and proportion of daily feeds provided as human milk up to 12 weeks 3. Haemoglobin concentration, serum phosphate and urea level at end of 4 months intervention period
Notes
If breast feeding was discontinued (or insufficient for all feeds) infants received either a formula milk (during first two months protein and mineral enriched milk, for the following two months, a standard ’term’ formula was used) By 2 months post term, 54 of 105 intervention group infants had changed nutrition, and 24 of 102 controls, and by 4 months post term, 85 of 105 intervention group infants had changed nutrition, and 57 of 102 controls Multiple birth siblings were randomised together: 42 of 105 (intervention) versus 27 of 102 (controls) were multiples The authors acknowledge that Mead Johnson Nutritionals donated nutritional products used in the trial
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
15
Zachariassen 2011
(Continued)
Risk of bias Bias
Authors’ judgement
Support for judgement
Random sequence generation (selection Low risk bias)
Computer-generated
Allocation concealment (selection bias)
Sequence stored in sealed envelopes
Low risk
Blinding (performance bias and detection High risk bias) All outcomes
Unblinded to parents, caregivers, and investigators
Incomplete outcome data (attrition bias) All outcomes
Near complete follow-up (97%)
Low risk
Characteristics of excluded studies [ordered by study ID]
Study
Reason for exclusion
Hall 1993
The intervention group received only mineral supplements. The trial did not report growth as an outcome
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
16
DATA AND ANALYSES
Comparison 1. Multinutrient fortification vs. no fortification of human breast milk
Outcome or subgroup title 1 Weight (g) 1.1 3-4 months corrected age 1.2 12 months corrected age 2 Head circumference (cm) 2.1 3-4 months corrected age 2.2 12 months corrected age 3 Length (cm) 3.1 3-4 months corrected age 3.2 12 months corrected age 4 Visual acuity (cycles/degree) 4.1 4 months corrected age 4.2 6 months corrected age 5 Contrast sensitivity (log) 5.1 4 months corrected age 5.2 6 months corrected age 6 Bone mineral content (g) 6.1 4 months corrected age 6.2 12 months corrected age 7 Bone mineral density (g/cm2 ) 7.1 4 months corrected age 7.2 12 months corrected age 8 Duration of human milk feeding 8.1 Postnatal weeks 8.2 Post discharge weeks 9 Proportion of infants fed with breast milk at end of intervention period 9.1 Exclusively fed with human milk 9.2 At least partially fed with human milk
No. of studies
No. of participants
2 2
236
Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI)
2
211
Mean Difference (IV, Fixed, 95% CI)
Statistical method
Effect size
Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Mean Difference (IV, Fixed, 95% CI) Risk Ratio (M-H, Fixed, 95% CI)
Subtotals only 138.26 [-89.87, 366. 40] 255.25 [-93.40, 603. 90] Subtotals only 0.22 [-0.15, 0.58] 0.16 [-0.27, 0.60] Subtotals only 0.60 [-0.14, 1.33] 0.88 [0.01, 1.74] Totals not selected 0.0 [0.0, 0.0] 0.0 [0.0, 0.0] Totals not selected 0.0 [0.0, 0.0] 0.0 [0.0, 0.0] Totals not selected 0.0 [0.0, 0.0] 0.0 [0.0, 0.0] Totals not selected 0.0 [0.0, 0.0] 0.0 [0.0, 0.0] Totals not selected 0.0 [0.0, 0.0] 0.0 [0.0, 0.0] Totals not selected
1
Risk Ratio (M-H, Fixed, 95% CI)
0.0 [0.0, 0.0]
1
Risk Ratio (M-H, Fixed, 95% CI)
0.0 [0.0, 0.0]
2 2 2 2 2 2 1 1 1 1 1 1 1 1 1 1 1 1 2 1 1 2
235 197 236 211
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
17
Analysis 1.1. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 1 Weight (g). Review:
Multinutrient fortification of human breast milk for preterm infants following hospital discharge
Comparison: 1 Multinutrient fortification vs. no fortification of human breast milk Outcome: 1 Weight (g)
Study or subgroup
Nutrient fortified
Mean Difference
Non-fortified
Weight
IV,Fixed,95% CI
Mean Difference
N
Mean(SD)
N
Mean(SD)
IV,Fixed,95% CI
17
5535 (766)
17
5042 (967)
15.1 %
493.00 [ -93.42, 1079.42 ]
Zachariassen 2011
104
6464 (951)
98
6389 (844)
84.9 %
75.00 [ -172.65, 322.65 ]
Subtotal (95% CI)
121
1 3-4 months corrected age O’Connor 2008
100.0 % 138.26 [ -89.87, 366.40 ]
115
Heterogeneity: Chi2 = 1.66, df = 1 (P = 0.20); I2 =40% Test for overall effect: Z = 1.19 (P = 0.23) 2 12 months corrected age O’Connor 2008
14 9835 (1152)
16 8648 (1438)
14.1 %
1187.00 [ 259.31, 2114.69 ]
Zachariassen 2011
92 9446 (1339)
89 9344 (1243)
85.9 %
102.00 [ -274.23, 478.23 ]
Subtotal (95% CI)
106
105
100.0 % 255.25 [ -93.40, 603.90 ]
Heterogeneity: Chi2 = 4.51, df = 1 (P = 0.03); I2 =78% Test for overall effect: Z = 1.43 (P = 0.15) Test for subgroup differences: Chi2 = 0.30, df = 1 (P = 0.58), I2 =0.0%
-1000
-500
Favours control
0
500
1000
Favours fortified
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
18
Analysis 1.2. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 2 Head circumference (cm). Review:
Multinutrient fortification of human breast milk for preterm infants following hospital discharge
Comparison: 1 Multinutrient fortification vs. no fortification of human breast milk Outcome: 2 Head circumference (cm)
Study or subgroup
Nutrient fortified
Mean Difference
Non-fortified
Weight
IV,Fixed,95% CI
Mean Difference
N
Mean(SD)
N
Mean(SD)
IV,Fixed,95% CI
17
40.5 (1)
17
39.3 (1.5)
18.0 %
1.20 [ 0.34, 2.06 ]
Zachariassen 2011
103
42.1 (1.6)
98
42.1 (1.3)
82.0 %
0.0 [ -0.40, 0.40 ]
Subtotal (95% CI)
120
1 3-4 months corrected age O’Connor 2008
100.0 % 0.22 [ -0.15, 0.58 ]
115
Heterogeneity: Chi2 = 6.17, df = 1 (P = 0.01); I2 =84% Test for overall effect: Z = 1.17 (P = 0.24) 2 12 months corrected age O’Connor 2008
14
47 (1.1)
16
46 (1.4)
24.1 %
1.00 [ 0.10, 1.90 ]
Zachariassen 2011
81
46.7 (1.8)
86
46.8 (1.5)
75.9 %
-0.10 [ -0.60, 0.40 ]
Subtotal (95% CI)
95
102
100.0 % 0.16 [ -0.27, 0.60 ]
Heterogeneity: Chi2 = 4.40, df = 1 (P = 0.04); I2 =77% Test for overall effect: Z = 0.73 (P = 0.46) Test for subgroup differences: Chi2 = 0.03, df = 1 (P = 0.86), I2 =0.0%
-2
-1
Favours fortified
0
1
2
Favours control
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
19
Analysis 1.3. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 3 Length (cm). Review:
Multinutrient fortification of human breast milk for preterm infants following hospital discharge
Comparison: 1 Multinutrient fortification vs. no fortification of human breast milk Outcome: 3 Length (cm)
Study or subgroup
Nutrient fortified
Mean Difference
Non-fortified
Weight
IV,Fixed,95% CI
Mean Difference
N
Mean(SD)
N
Mean(SD)
IV,Fixed,95% CI
17
59 (2.7)
17
56.7 (3)
14.8 %
2.30 [ 0.38, 4.22 ]
Zachariassen 2011
104
63 (2.9)
98
62.7 (2.9)
85.2 %
0.30 [ -0.50, 1.10 ]
Subtotal (95% CI)
121
1 3-4 months corrected age O’Connor 2008
100.0 % 0.60 [ -0.14, 1.33 ]
115
Heterogeneity: Chi2 = 3.56, df = 1 (P = 0.06); I2 =72% Test for overall effect: Z = 1.58 (P = 0.11) 2 12 months corrected age O’Connor 2008
14
76.5 (2.9)
16
72.7 (4.2)
11.4 %
3.80 [ 1.24, 6.36 ]
Zachariassen 2011
92
75.5 (3.1)
89
75 (3.2)
88.6 %
0.50 [ -0.42, 1.42 ]
100.0 %
0.88 [ 0.01, 1.74 ]
Subtotal (95% CI)
106
105
Heterogeneity: Chi2 = 5.66, df = 1 (P = 0.02); I2 =82% Test for overall effect: Z = 1.99 (P = 0.047) Test for subgroup differences: Chi2 = 0.23, df = 1 (P = 0.63), I2 =0.0%
-10
-5
Favours control
0
5
10
Favours fortified
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
20
Analysis 1.4. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 4 Visual acuity (cycles/degree). Review:
Multinutrient fortification of human breast milk for preterm infants following hospital discharge
Comparison: 1 Multinutrient fortification vs. no fortification of human breast milk Outcome: 4 Visual acuity (cycles/degree)
Study or subgroup
Nutrient fortified
Mean Difference
Non-fortified
Mean Difference
N
Mean(SD)
N
Mean(SD)
IV,Fixed,95% CI
IV,Fixed,95% CI
16
7.8 (1.3)
16
6.9 (1.2)
0.90 [ 0.03, 1.77 ]
14
9.7 (1.2)
17
8.2 (1.3)
1.50 [ 0.62, 2.38 ]
1 4 months corrected age O’Connor 2008 2 6 months corrected age O’Connor 2008
-2
-1
0
Favours control
1
2
Favours fortified
Analysis 1.5. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 5 Contrast sensitivity (log). Review:
Multinutrient fortification of human breast milk for preterm infants following hospital discharge
Comparison: 1 Multinutrient fortification vs. no fortification of human breast milk Outcome: 5 Contrast sensitivity (log)
Study or subgroup
Nutrient fortified
Mean Difference
Non-fortified
Mean Difference
N
Mean(SD)
N
Mean(SD)
IV,Fixed,95% CI
IV,Fixed,95% CI
10
1.8 (0.3)
12
1.7 (0.2)
0.10 [ -0.12, 0.32 ]
11
2 (0.3)
15
1.9 (0.2)
0.10 [ -0.10, 0.30 ]
1 4 months corrected age O’Connor 2008 2 6 months corrected age O’Connor 2008
-0.2
-0.1
Favours control
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
0
0.1
0.2
Favours fortified
21
Analysis 1.6. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 6 Bone mineral content (g). Review:
Multinutrient fortification of human breast milk for preterm infants following hospital discharge
Comparison: 1 Multinutrient fortification vs. no fortification of human breast milk Outcome: 6 Bone mineral content (g)
Study or subgroup
Nutrient fortified
Mean Difference
Non-fortified
Mean Difference
N
Mean(SD)
N
Mean(SD)
IV,Fixed,95% CI
IV,Fixed,95% CI
17
75.4 (15)
17
54.8 (25.8)
20.60 [ 6.41, 34.79 ]
13
185.8 (29.1)
14
156 (39.8)
29.80 [ 3.63, 55.97 ]
1 4 months corrected age O’Connor 2008 2 12 months corrected age O’Connor 2008
-50
-25
0
25
Favours control
50
Favours fortified
Analysis 1.7. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 7 Bone mineral density (g/cm2 ). Review:
Multinutrient fortification of human breast milk for preterm infants following hospital discharge
Comparison: 1 Multinutrient fortification vs. no fortification of human breast milk Outcome: 7 Bone mineral density (g/cm2 )
Study or subgroup
Nutrient fortified
Mean Difference
Non-fortified
Mean Difference
N
Mean(SD)
N
Mean(SD)
IV,Fixed,95% CI
IV,Fixed,95% CI
17
0.477 (0.026)
17
0.47 (0.025)
0.00 [ -0.01, 0.02 ]
13
0.594 (0.034)
14
0.58 (0.03)
0.02 [ -0.01, 0.04 ]
1 4 months corrected age O’Connor 2008 2 12 months corrected age O’Connor 2008
-0.05
-0.03
Favours control
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
0
0.03
0.05
Favours fortified
22
Analysis 1.8. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 8 Duration of human milk feeding. Review:
Multinutrient fortification of human breast milk for preterm infants following hospital discharge
Comparison: 1 Multinutrient fortification vs. no fortification of human breast milk Outcome: 8 Duration of human milk feeding
Study or subgroup
Nutrient fortified
Mean Difference
Non-fortified
Mean Difference
N
Mean(SD)
N
Mean(SD)
IV,Fixed,95% CI
IV,Fixed,95% CI
13
43.3 (17.7)
17
51.5 (12.4)
-8.20 [ -19.48, 3.08 ]
105
10.6 (7.5)
102
11.8 (7.7)
-1.20 [ -3.27, 0.87 ]
1 Postnatal weeks O’Connor 2008 2 Post discharge weeks Zachariassen 2011
-20
-10
0
Favours control
10
20
Favours fortified
Analysis 1.9. Comparison 1 Multinutrient fortification vs. no fortification of human breast milk, Outcome 9 Proportion of infants fed with breast milk at end of intervention period. Review:
Multinutrient fortification of human breast milk for preterm infants following hospital discharge
Comparison: 1 Multinutrient fortification vs. no fortification of human breast milk Outcome: 9 Proportion of infants fed with breast milk at end of intervention period
Study or subgroup
Nutrient fortified
Non-fortified
n/N
n/N
Risk Ratio
Risk Ratio
20/105
38/95
0.48 [ 0.30, 0.76 ]
15/17
16/17
0.94 [ 0.76, 1.16 ]
M-H,Fixed,95% CI
M-H,Fixed,95% CI
1 Exclusively fed with human milk Zachariassen 2011 2 At least partially fed with human milk O’Connor 2008
0.5
0.7
Favours control
1
1.5
2
Favours fortifiied
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
23
WHAT’S NEW Last assessed as up-to-date: 10 September 2012.
Date
Event
Description
14 March 2013
Amended
Text correction in Plain Language Summary
HISTORY Protocol first published: Issue 3, 2004 Review first published: Issue 4, 2007
Date
Event
Description
10 September 2012
New citation required and conclusions have changed
Search was updated in August 2012. New author added. One new trial included (Zachariassen 2011).
10 September 2012
New search has been performed
This updates the review ’Multrinutrient fortification of human breast milk for preterm infants following hospital discharge’ (McCormick 2010).
14 May 2010
New citation required and conclusions have changed
April 2010 search found one trial for inclusion ( O’Connor 2008).
14 May 2010
New search has been performed
The review title and description of intervention have been amended at this update to ”Multinutrient fortification of human breast milk for preterm infants following hospital discharge“ This review was previously titled ’Multicomponent fortification of human breast milk for preterm infants following hospital discharge” (Henderson 2007).
22 August 2008
Amended
Converted to new review format.
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
24
CONTRIBUTIONS OF AUTHORS Lauren Young, Nick Embleton, Felicia McCormick, William McGuire undertook the electronic search and identified citations for possible inclusion. Lauren Young, Nick Embleton and Felicia McCormick reviewed the citation list (title and abstract) for inclusion and undertook methodological appraisal, data extraction, entry and analysis. William McGuire acted as an arbiter for any disagreements, reviewed data entry and analysis and completed the review.
DECLARATIONS OF INTEREST None
SOURCES OF SUPPORT Internal sources • CRD & Hull York Medical School, University of York, UK.
External sources • NIHR, UK. LY is an NIHR academic clinical fellow. • Eunice Kennedy Shriver National Institute of Child Health and Human Development National Institutes of Health, Department of Health and Human Services, USA. The Cochrane Neonatal Review Group has been funded in part with Federal funds from the Eunice Kennedy Shriver National Institute of Child Health and Human Development National Institutes of Health, Department of Health and Human Services, USA, under Contract No. HHSN267200603418C
INDEX TERMS Medical Subject Headings (MeSH) ∗ Food,
Fortified; ∗ Milk, Human; Aftercare [∗ methods]; Infant, Low Birth Weight; Infant, Newborn; Infant, Premature [∗ growth & development]; Patient Discharge; Randomized Controlled Trials as Topic
MeSH check words Humans; Infant
Multinutrient fortification of human breast milk for preterm infants following hospital discharge (Review) Copyright © 2013 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
25