Malignant pulmonary and mediastinal tumors in children: differential diagnoses M.B. McCarville Author information ► Copyright and License information ► This article has been cited by other articles in PMC.
Go to:
Abstract article-meta Conventional chest radiography is the most common imaging procedure in children. When a chest mass is discovered, crosssectional imaging is often required to accurately localize and characterize the lesion in order to narrow the differential diagnosis. Knowledge of the differential diagnostic possibilities for chest tumors in children is important for both the pediatric and general radiologist because they differ from adults. The more common pediatric, malignant, mediastinal and pulmonary tumors and the characteristic imaging and clinical features that are useful in distinguishing between them are discussed in this review. Keywords: Pleuropulmonary blastoma, lymphoma, germ cell tumor, neuroblastoma, Askin tumor, sarcoma Go to:
Malignant mediastinal tumors Tumors in the mediastinum are best characterized by the compartment in which they arise. Malignant tumors arising in the anterior mediastinum are most commonly due to lymphoma or leukemia followed by germ cell tumors. Malignant tumors of the middle mediastinum are usually due to adenopathy from leukemia or lymphoma. Middle mediastinal tumors are usually seen in association with anterior mediastinal disease. They are rarely seen in isolation. Tumors of the posterior mediastinum are usually of neurogenic origin with neuroblastoma being most common. Lymphoma and leukemia
Lymphoma accounts for approximately 13% of all childhood cancers and is the most common cause of a mediastinal mass in
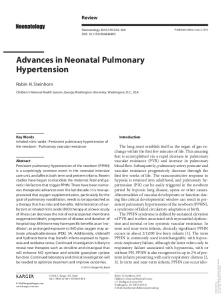
children. Sixty percent of all lymphomas in this age group are nonHodgkin lymphomas and Hodgkin lymphomas make up the remainder. Although non-Hodgkin lymphoma is more common, about half of the children with non-Hodgkin lymphoma and twothirds of those with Hodgkin lymphoma present with an anterior mediastinal mass. Therefore, most anterior mediastinal masses in children are due to Hodgkin lymphoma[1,2]. In most cases the anterior mediastinal mass is due to infiltration of the thymus, although enlarged mediastinal nodes are often present. The thymus and nodes are often very necrotic[3]. Direct invasion of the pericardium can lead to pericardial effusion, a well-known phenomenon in Hodgkin lymphoma. Direct invasion of the chest wall may also occur. The size of the mediastinal mass and the mediastinal/thoracic ratio, measured on a posterior–anterior radiograph, have implications for prognosis and risk stratification in children with Hodgkin disease. The mediastinal mass may compress and compromise the trachea and superior vena cava. When the trachea is compressed to <50% of its normal diameter, patients should not be sedated or anesthetized because of the risk of airway obstruction[4,5]. Associated pulmonary nodules and pleural effusions occur in only about 5% of patients with Hodgkin lymphoma, whereas effusions occur in 50–75% of those with lymphoblastic lymphoma (Fig. 1)[1,2]. T-cell leukemia and lymphoblastic lymphoma are closely related and patients with T-cell leukemia may present with an anterior mediastinal mass and pleural effusions. The distinction between the two is arbitrarily based on the degree of bone marrow involvement such that patients with ≥25% marrow blasts are designated as having leukemia[6]. fig ft0fig mode=article f1
Figure 1 caption a4 A 13-year-old boy with T-cell, lymphoblastic lymphoma. (A) Axial CT image shows a lobulated anterior mediastinal mass (arrows) and (B) pericardial (straight arrow) and pleural effusions (curved arrow). Pericardial and pleural effusions are commonly seen ... Malignant germ cell tumors
Germ cell tumors (GCT) account for 6–18% of mediastinal masses and mediastinal primary GCTs account for 1–3% of all GCTs[3]. About 20% of mediastinal GCTs are malignant and include seminomas and non-seminomatous tumors such as teratocarcinoma, yolk sac tumor, embryonal carcinoma, choriocarcinoma, and mixed types. Malignant GCT is generally a complex tumor often containing coexisting benign components. There are two age peaks for mediastinal GCTs: at about 2 years of age and adolescence. Most malignant GCTs occur in adolescent boys. Mediastinal GCTs are often large and cause respiratory distress as a result of compression of the tracheobronchial tree. Patients often present with diminished breath sounds, pain and cough[7]. Mediastinal GCTs most often arise within or near the thymus but may also originate within the heart or pericardium and rarely in the posterior mediastinum[7]. Benign and malignant GCTs contain calcification (33–50%), fat and cystic or necrotic areas (Fig. 2). Malignant tumors tend to be large, cause a marked mass effect and infiltrate adjacent structures. Seminomas rarely calcify and are typically homogeneous tumors. Non-seminomatous GCTs are
invasive tumors that are inhomogeneous and contain areas of necrosis and hemorrhage[8]. Seminomas lack serologic markers, whereas non-seminomatous tumors are often associated with increased serum β-human chorionic gonadotropin or alphafetoprotein levels that can induce precocious puberty and may be associated with Klinefelter syndrome. Seminomas require histologic diagnosis, whereas non-seminomatous tumors can be diagnosed by serum markers and clinical and radiological correlation[8]. fig ft0fig mode=article f1
Figure 2 caption a4 A 2-year-old malignant G a 2-month h increased w fever and ni serum alpha was marked Posterior-an showing larg ... Neurogenic tumors
Approximately 90% of posterior mediastinal masses in children are of neurogenic origin[1,9]. These include ganglion cell tumors, nerve
sheath and nerve tumors, and other nervous tissue tumors such as paragangliomas[3]. Most posterior mediastinal tumors in children are ganglion cell tumors. These tumors arise from sympathetic chain ganglia and form a spectrum of disease ranging from the most aggressive, neuroblastoma, to the less aggressive, ganglioneuroblastoma and benign ganglioneuroma[1]. Neuroblastoma occurs at a median age of 2 years, ganglioneuroblastoma at a median age of 5.5 years and ganglioneuroma usually occurs after 10 years of age. All three have similar radiologic features. On conventional radiography these tumors appear as a vertically elongated mass with tapered superior and inferior margins (Fig. 3). The lateral margin is usually smooth and convex. About 30% contain calcification. Bone changes include spreading and erosion of ribs and widening of neural foramina[3]. fig ft0fig mode=article f1
Figure 3 A 3-week-old boy with posterior mediastinal neuroblastoma. (A) Posterior-anterior chest radiograph shows a sharply circumscribed left paraspinal mass (arrows) initially thought to represent round pneumonia. (B) Axial CT image shows a solid mass (arrow) ...The clinical presentation of neuroblastoma ranges from clinically silent to symptoms associated with disseminated disease such as irritability, diarrhea, weight loss, fever and bone pain[1]. A local mass effect or intraspinal tumor extension can cause respiratory distress or cord compression[3]. When neuroblastoma occurs near the lung apex or base of the neck, it can cause Horner syndrome (ptosis, myosis, anhydrosis). Opsoclonus-myoclonus, a syndrome characterized by rapid eye movements, occurs rarely. Patients with opsoclonus-myoclonus typically have tumors with favorable
Figure 3 caption a4
biological behavior but suffer from long-term neurologic sequelae. Nerve sheath tumors consist of schwannomas, encapsulated tumors lacking nerve fibers, and neurofibromas, non-encapsulated tumors with nerve fibers. These tumors may arise from intercostal or sympathetic nerves. Radiologically, the tumors are indistinguishable and usually appear as sharply marginated, spherical and lobulated paraspinal masses. Rib erosion and splaying of ribs is more commonly seen with nerve sheath tumors than ganglion tumors. About 10% will have intraspinal extension. On magnetic resonance imaging (MRI), T1-weighted sequences both have a homogeneous signal. On axial T2-weighted sequences they exhibit a target sign, with high signal intensity at the periphery and intermediate signal centrally. About 5% of these tumors undergo malignant degeneration and about half of these are seen in patients with type 1 neurofibromatosis[3,10]. Malignant peripheral nerve sheath tumors are typically larger than their benign counterpart and demonstrate rapid growth with central necrosis[10]. Go to:
Pulmonary and chest wall malignancies In children, most pulmonary malignancies are metastatic in nature[9,11]. It is difficult to distinguish benign from malignant pulmonary nodules in children, based on computed tomographic imaging features[11,12]. Although pulmonary metastases often appear as round, sharply marginated nodules, they may be illdefined. Unlike in adults, nodule size is not a useful indicator of malignant potential in children and nodules <0.5 cm seem to be as likely to be malignant as those >0.5 cm[11]. The most common pulmonary malignancies in children are carcinoid tumor and pleuropulmonary blastoma[13]. Askin tumor is a round cell tumor in the Ewing sarcoma family of tumors that arises in the chest wall of children[14]. Carcinoid tumor
Carcinoid tumor occurs in older children and adolescents and has been reported to account for 80% to 85% of primary malignant lung tumors in children. These tumors arise in the lobar bronchi (75%),
main stem bronchi (10%) or within the lung parenchyma (15%). Patients present with wheezing, cough, hemoptysis or recurrent pneumonia[13]. Chest radiographs often show a hilar or perihilar mass in isolation or in association with a peripheral consolidation due to atelectasis or obstructive pneumonia. On computed tomography (CT), carcinoid generally appears as a round or ovoid solid, well-defined mass with slightly lobulated margins (Fig. 4). When non-spherical they may appear elongated with the long axis parallel to the bronchi or pulmonary vessels. They typically occur close to the central bronchi, near the bifurcation. On CT, calcification is present in up to 30% of tumors and may be punctate or diffuse. Calcification is more common in central carcinoid than peripheral carcinoid. Carcinoids may manifest as a small nodule entirely located within the lumen of a bronchus or with endobronchial and extrabronchial components. Thin-section CT is useful in identifying the endobronchial component. Carcinoids tend to be vascular and may demonstrate intense enhancement on CT imaging. This feature is useful in distinguishing between carcinoid tumor and a mucous plug[15]. fig ft0fig mode=article f1
Figure 4 An 11-year-old boy with pulmonary carcinoid. (A) Axial CT image shows a sharply defined, round mass in or adjacent to the right main stem bronchus (arrow) causing partial bronchial obstruction. Note enhancement of the mass, a feature typical of carcinoid. ...Pleuropulmonary blastoma Pleuropulmonary blastoma (PPB) is a rare malignant embryonal mesenchymal tumor of the lung and pleura that occurs almost exclusively in children younger than 6 years of age. There are three subtypes of PPB: type 1 is predominantly macrocystic (14%), type 2 is mixed cystic and solid (48%) and type 3 is predominantly solid
(38%). The diagnosis is often delayed because they are confused with other tumors, especially cystic adenomatoid malformation, or empyema. Patients present with non-specific respiratory distress or signs of pneumonia and spontaneous pneumothorax. Although PPB has not been identified as part of a specific syndrome, about 25% of cases occur in a familial setting with a high prevalence of extrapulmonary tumors including cystic nephroma (most common), thyroid neoplasms, sarcomas, medulloblastoma, GCT and hematologic disease. Because the diagnosis is often delayed patients tend to present with large masses causing near complete opacification of the hemithorax (Fig. 5). Other imaging features that suggest PPB are right-sided location, peripherally located mass without chest wall invasion, heterogeneously low attenuation on CT, lack of calcification and associated pleural effusion and pneumothorax[16,17]. Pleuropulmonary blastoma may be solitary or multiple with additional lesions occurring synchronously or metachronously[13]. The presence of multiple lesions should suggest the diagnosis of PPB. fig ft0fig mode=article f1
Figure 5 A 2-year-old girl with pleuropulmonary blastoma (PPB). (A) Posterior-anterior chest radiograph shows complete opacification of the right hemithorax. (B) Axial CT, lung window, shows a small right pneumothorax. (C) Axial CT, mediastinal window, shows the ...Askin tumor Askin tumor is a Ewing sarcoma or primitive neuroectodermal tumor that arises from the chest wall, occasionally from a rib and rarely from lung parenchyma. About 17% of malignant tumors of the chest are of the Ewing sarcoma family of tumors and 15% of all
Ewing sarcomas are localized to the chest wall[14,18]. Ewing sarcoma may occur in any age group but the median age of presentation is 15 years. The most common presenting symptom is localized pain followed by a palpable mass[19]. The prognosis of patients with Askin tumor is poor and depends on tumor extension at diagnosis and tumor resectability after neoadjuvant therapy[18]. The tumor often presents as a large chest wall mass with an intrathoracic or extrathoracic component or both. Rapid growth of these tumors results in invasion and destruction of adjacent structures, including muscle, ribs, pleura and lung parenchyma. It can be difficult to distinguish between lung compression and invasion by CT or MRI. Tumor extension into the pleura and pleural effusions occur frequently. Rib destruction is common (Fig. 6). Askin tumor rarely contains calcification. The tumors usually have a heterogeneous appearance on CT and MRI caused by necrosis and hemorrhage[18,20,21]. fig ft0fig mode=article f1
Figure 6 A 3-year-old girl with Askin tumor. (A) Axial CT image shows a large heterogeneous Askin tumor (arrows) with associated rib destruction (curved arrow). (B) Coronal CT reconstruction shows a heterogeneous Askin tumor (arrows) and large associated pleural ...Go to: References [1] Meza MP, Benson M, Slovis TL. Imaging of mediastinal masses
in children. Radiol Clin North Am. 1993;31:583–604. [PubMed] [2] Parker BR. Leukemia and lymphoma in childhood. Radiol Clin North Am. 1997;35:1495–516. [PubMed] [3] Franco A, Mody NS, Meza MP. Imaging evaluation of pediatric mediastinal masses. Radiol Clin North Am. 2005;43:325–53. doi:10.1016/j.rcl.2005.01.002. PMid:15737372. [PubMed] [4] Shamberger RC. Preanesthetic evaluation of children with anterior mediastinal masses. Semin Pediatr Surg. 1999;8:61–8. [PubMed] [5] Lam JC, Chui CH, Jacobsen AS, Tan AM, Joseph VT. When is a mediastinal mass critical in a child? An analysis of 29 patients. Pediatr Surg Int. 2004;20:180–4. doi:10.1007/s00383-004-1142-6. PMid:15064964. [PubMed] [6] Link M. Malignant non-Hodgkin lymphomas in children. In: Pizzo PA, Poplack DG, editors. Principles and practice of pediatric oncology. 6th. Philadelphia: Lippincott, Williams and Wilkins; 2010. pp. 725–33. [7] Barksdale EM, Jr, Obokhare I. Teratomas in infants and children. Curr Opin Pediatr. 2009;21:344–9. doi:10.1097/MOP.0b013e32832b41ee. PMid:19417664. [PubMed] [8] Wright CD. Mediastinal tumors and cysts in the pediatric population. Thorac Surg Clin. 2009;19:47–61, vi. doi:10.1016/j.thorsurg.2008.09.014. PMid:19288820. [PubMed] [9] Wyttenbach R, Vock P, Tschappeler H. Cross-sectional imaging with CT and/or MRI of pediatric chest tumors. Eur Radiol. 1998;8:1040–6. doi:10.1007/s003300050511. PMid:9683716. [PubMed] [10] Wu JS, Hochman MG. Soft-tissue tumors and tumorlike lesions: a systematic imaging approach. Radiology. 2009;253:297– 316. doi:10.1148/radiol.2532081199. PMid:19864525. [PubMed] [11] McCarville MB, Lederman HM, Santana VM, et al. Distinguishing benign from malignant pulmonary nodules with helical chest CT in children with malignant solid tumors. Radiology. 2006;239:514–20. doi:10.1148/radiol.2392050631. PMid:16641356. [PubMed]
[12] Silva CT, Amaral JG, Moineddin R, Doda W, Babyn PS. CT characteristics of lung nodules present at diagnosis of extrapulmonary malignancy in children. AJR Am J Roentgenol. 2010;194:772–8. doi:10.2214/AJR.09.2490. PMid:20173158. [PubMed] [13] Dishop MK, Kuruvilla S. Primary and metastatic lung tumors in the pediatric population: a review and 25-year experience at a large children's hospital. Arch Pathol Lab Med. 2008;132:1079–103. [PubMed] [14] Laskar S, Nair C, Mallik S, et al. Prognostic factors and outcome in Askin–Rosai tumor: a review of 104 patients. Int J Radiat Oncol Biol Phys. 2010 doi:10.1016/j.ijrobp.2009.10.039. [PubMed] [15] Chong S, Lee KS, Chung MJ, Han J, Kwon OJ, Kim TS. Neuroendocrine tumors of the lung: clinical, pathologic, and imaging findings. Radiographics. 2006;26:41–57. doi:10.1148/rg.261055057. PMid:16418242. [PubMed] [16] Papaioannou G, Sebire NJ, McHugh K. Imaging of the unusual pediatric ‘blastomas’ Cancer Imaging. 2009;9:1–11. doi:10.1102/1470-7330.2009.0001. PMid:19237343. [PMC free article] [PubMed] [17] Naffaa LN, Donnelly LF. Imaging findings in pleuropulmonary blastoma. Pediatr Radiol. 2005;35:387–91. doi:10.1007/s00247-0041367-5. PMid:15657793. [PubMed] [18] Sallustio G, Pirronti T, Lasorella A, Natale L, Bray A, Marano P. Diagnostic imaging of primitive neuroectodermal tumour of the chest wall (Askin tumour) Pediatr Radiol. 1998;28:697–702. doi:10.1007/s002470050443. PMid:9732497. [PubMed] [19] Bernstein M, Kovar H, Paulussen M, et al. Ewing sarcoma family of tumors: Ewing sarcoma of bone and soft tissue and the peripheral primitive neuroectodermal tumors. In: Pizzo PA, Poplack DG, editors. Principles and practice of pediatric oncology. 5th ed. Philadelphia: Lippincott, Williams and Wilkins; 2005. pp. 1002–32. [20] Winer-Muram HT, Kauffman WM, Gronemeyer SA, Jennings SG. Primitive neuroectodermal tumors of the chest wall (Askin
tumors): CT and MR findings. AJR Am J Roentgenol. 1993;161:265–8. [PubMed] [21] Dick EA, McHugh K, Kimber C, Michalski A. Imaging of noncentral nervous system primitive neuroectodermal tumours: diagnostic features and correlation with outcome. Clin Radiol. 2001;56:206–15. doi:10.1053/crad.2000.0614. PMid:11247698. [PubMed]