Gynecologic Oncology 83, 472– 476 (2001) doi:10.1006/gyno.2001.6427, available online at http://www.idealibrary.com on
Pulmonary Resection in Metastatic Uterine and Cervical Malignancies Timothy M. Anderson, M.D., 1 John J. McMahon, M.D., Chukwumere E. Nwogu, M.D., Mathew W. Pombo, John D. Urschel, M.D., Deborah L. Driscoll, B.A., and Shashikant B. Lele, M.D. Roswell Park Cancer Institute and SUNY at Buffalo, Department of Surgical Oncology, Buffalo, New York 14263 Received May 15, 2001; published online October 31, 2001
are significant, and observed median survivals are less than 12 months [3]. The estimated number of new cervical cancers is 12,800, with 4600 dying of their disease. In cancer of the cervix, chemotherapy has been used for recurrent or metastatic disease, but has a limited influence on survival [4]. Clearly we are in need of better treatment options for advanced stage uterine and cervical malignancies. The role of surgery for lung metastasis has been well defined in a variety of solid tumors [5]. However, within the vast array of pulmonary metastasectomy literature gynecologic cancers are often lumped with “other” tumors and warrant more individualized delineation.
Objective. Although thoracotomy for removal of pulmonary metastasis is well documented in a wide variety of solid tumors, data are sparse regarding management of patients with gynecologic malignancies metastatic to the lung. Methods. We retrospectively reviewed the Roswell Park Cancer Institute experience between 1982 and 1999. Of 82 eligible patients with gynecologic tumors metastatic and confined to the lung, 25 underwent pulmonary resection. Results. There were 60 uterine and 22 cervix cancer patients with pulmonary metastases. Among patients with uterine cancer primaries undergoing pulmonary resection (n ⴝ 19) median survival was 26 months. Uterine cancer patients who underwent surgical resection for leiomyosarcomas (n ⴝ 11) had a median survival of 25 months compared to 46 months in patients with adenocarcinoma (n ⴝ 6, P ⴝ 0.02). Median survival in cervix cancer patients undergoing resection for pulmonary metastases (n ⴝ 6) was 36 months. Conclusions. Pulmonary resection may provide a survival advantage for selected patients with uterine and cervical malignancies with metastases isolated to the lung. © 2001 Academic Press Key Words: uterine; cervix; cancer; pulmonary metastases; surgery.
MATERIALS AND METHODS
INTRODUCTION
An analysis of cervical and uterine malignancies metastatic to the lung was performed by IRB-approved retrospective review of charts for patients seen at Roswell Park Cancer Institute between January 1, 1982, and July 20, 1999. A total of 989 uterine and 1025 cervical cancer patients were treated for their primary cancer. Among these, 60 uterine (6.1%) and 22 cervical (2.1%) cancer patients had metastases isolated to the lung at the time of referral. Age, stage (FIGO), primary treatment, histology, disease-free interval (DFI), unilateral versus bilateral disease, pulmonary procedures, completeness of resection, number of lesions, and survival (interval from lung resection until death or last follow-up) were compared. Initial treatment for all uterine primary tumors had included total abdominal hysterectomy and bilateral salpingo-oophorectomy. In cervical patients undergoing lung surgery, 5 patients initially had hysterectomy and 1 received primary radiation therapy to the pelvis. In the cervical nonoperative group 14 patients underwent hysterectomy whereas 2 received primary radiation therapy. There were 82 patients with either cervical (22 patients) or uterine (60 patients) tumors metastatic to the lungs. Twentyfive patients were selected for pulmonary resection, including 19 patients with uterine and 6 with cervical tumors. Patients with pulmonary metastases had received prior chemotherapy. Lung resection was performed because the isolated pulmonary disease either remained stable or progressed.
The estimated number of new uterine cancers in the United States in 2000 is 36,100, of whom 6500 will die. Uterine cancers are the fourth most common cancer in females (6%) and the eighth most common cause of cancer deaths (2%) in the United States [1]. Stage IV uterine cancer includes spread to adjacent organs, with distant metastases constituting 2.9% of cases [2]. Hematogenous metastasis most commonly involves the lung, but the liver, brain, bone, and other sites can be involved. In advanced stage IV uterine cancer chemotherapy has been given in various combinations with response rates up to 51%. However, the duration of response is brief, toxicities 1
To whom reprint requests should be addressed at Division of Thoracic Surgical Oncology, Roswell Park Cancer Institute, Elm & Carlton Streets, Buffalo, NY 14263. Fax: 716-845-7692. E-mail: Timothy.Anderson@ RoswellPark.org. 0090-8258/01 $35.00 Copyright © 2001 by Academic Press All rights of reproduction in any form reserved.
472
473
PULMONARY RESECTION IN UTERINE AND CERVICAL METASTASES
TABLE 1 Histology of Uterine and Cervix Malignancies
Adenocarcinoma Leiomyosarcoma Squamous cell carcinoma Mixed mesodermal sarcoma Stromal sarcoma
TABLE 3 Number of Pulmonary Metastases
Uterine
Cervix
6 11 0 1 1
2 0 4 0 0
There were 41 uterine and 16 cervical cancer patients who had their lung metastases treated nonoperatively. Patients were treated medically because they refused surgery, were medically inoperable, had multiple pulmonary metastases thought to be unresectable, had additional metastases found at extrapulmonary sites, or were felt to have too short a DFI. Uterine cancer patients received chemotherapy and/or progestational agents. All 16 cervix cancer patients received chemotherapy. Statistical Analysis Estimated survival distributions were calculated by the method of Kaplan and Meier [6]. Tests of significance with respect to survival distributions were based on the log-rank test [7]. Demographics comparing groups were based on the 2 [7] and Mann–Whitney tests [8]. RESULTS At the time of lung resection patients with uterine cancer had a median age of 60 years (range 39 –79). The median age of cervix cancer patients receiving lung surgery was 56 years (range 31–74). Histologies of uterine and cervix cancers are seen in Table 1. The majority of uterine cancer patients had either adenocarcinoma or leiomyosarcoma. Cervix cancer cell types included squamous cell carcinoma and adenocarcinoma. Operative approaches in patients with uterine malignancies TABLE 2 Thoracic Procedures Uterine
Wedge (s) Lobectomy Lobectomy/wedge Bilobectomy Segmentectomy Segmentectomy/wedge
Cervix
Initial
Redo
Initial
Redo
12 2 3 1 1 0
3a 2 0 0 0 1
4 2 0 0 0 0
2 0 0 0 0 0
Uterine Cervix
Two–three
Four⫹
6 1
10 4
3 1
Note. One, two–three, and four⫹ refer to the number of pulmonary metastases.
included three median sternotomies and 16 thoracotomies. In the uterine patients, there were 5 reoperations and 1 patient required a third wedge resection (Table 2). Two cervix cancer patients required repeat thoracotomy for subsequent disease. In patients with uterine cancer undergoing surgery, 10 had unilateral metastases, whereas 9 patients developed bilateral disease. In cervix cancer patients undergoing surgery, equal numbers of unilateral and bilateral disease were noted (3 each). We grouped patients according to the number of pulmonary metastases as seen in Table 3. The majority of patients undergoing pulmonary resection had one to three lesions. There was no 30-day surgical mortality. There were two major morbidities including reoperation for bleeding after a left lower lobectomy through a median sternotomy and a streptococcal pneumonia. Minor complications included urinary tract infection (two patients), prolonged air leak after a bilobectomy, and pneumothorax after chest tube removal requiring reinsertion (one patient each). DFI from the time of primary tumor treatment until lung resection for uterine cancer patients was a median of 33 months. DFI in cervix cancer patients treated surgically was 23 months. Comparing DFI and survival (Table 4), there were trends toward increased survival with greater DFI in uterine cancer patients. In patients undergoing lung surgery for metastatic uterine leiomyosarcoma (n ⫽ 11) postthoracotomy median survival was 25 months compared to 46 months in patients with adenocarcinoma (n ⫽ 6, P ⫽ 0.02). Median survival for uterine cancer patients undergoing surTABLE 4 Uterine Cancer DFI and Survival from Time of Lung Resection until Death or Last Follow-Up DFI (months)
Median months
2-Year survival
5-Year survival
0–11
23 (n ⫽ 3) 26 (n ⫽ 8) 30 (n ⫽ 8)
33%
0%
63%
13%
58%
0%
12–35 36⫹
Note. Initial and redo (operation) procedures. a One of the uterine cancer patients required a second reoperation for subsequent disease.
One
Note. Two- and 5-year survivals are estimated survivals.
474
ANDERSON ET AL.
TABLE 5 Uterine Cancer Patient Survival According to Number of Pulmonary Lesions Resected No. of lesions 1 2–3 4⫹
Median months
2-Year survival
5-Year survival
19 (n ⫽ 6) 35 (n ⫽ 10) 16 (n ⫽ 3)
33%
0%
79%
15%
33%
0%
Note. Two- and 5-year survivals are estimated survivals.
gery for unilateral metastases was 23 months compared to 35 months with bilateral disease. Median survival for cervix cancer patients undergoing surgery for unilateral pulmonary metastases was 45 months compared to 36 months for patients with bilateral disease. In uterine cancer patients, survival after resection of a single pulmonary metastasis (Table 5) was a median of 19 months, for 2–3 lesions 35 months, and for 4⫹ lesions 16 months. In cervix cancer patients median survival for resection of 1 lesion (n ⫽ 1) was 36 months, for 2–3 lesions (n ⫽ 4) 45 months, and for 4⫹ lesions (n ⫽ 1) 8 months. Among 13 uterine cancer patients undergoing complete resections (no evidence of residual disease and negative margins), median survival was 26 months compared to 18 months if they were incompletely resected (n ⫽ 6). Median survival in cervix cancer patients completely resected (n ⫽ 5) was 36 months compared to 8 months survival in the only patient incompletely resected (P ⫽ 0.02).
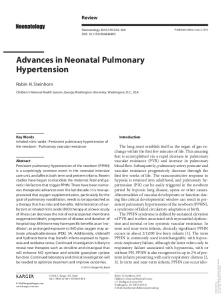
FIG. 1.
In the uterine cancer patients, median survival was 26 months (Fig. 1) after undergoing lung surgery (n ⫽ 19). In cervix cancer patients (n ⫽ 6), postthoracotomy median survival was 36 months (Fig. 2). DISCUSSION The first case describing resection of a pulmonary metastasis occurred in 1882 when two incidental pulmonary nodules were removed during a chest wall resection for sarcoma [9]. Several sporadic case reports of metastasectomy followed until 1947, when Alexander and Haight reported a series of 24 patients who had undergone resection for pulmonary metastasis. These authors also established the first criteria for pulmonary metastasectomy [5]. Since then criteria have been modified into almost universally accepted indications for pulmonary metastasectomy including (1) the ability to tolerate the procedure, (2) sufficient pulmonary reserve to compensate for the loss of lung capacity, (3) the site of primary must be controlled or controllable, (4) no evidence of extrapulmonary disease, and (5) no better therapy available [9 –12]. Among our uterine cancer patients 6.1% were found to have isolated lung metastasis. The lung is the most common organ involved in hematogenous uterine cancer spread [13]. Less common sites of metastatic spread include the liver, brain, and bone [2]. Our cervical cancer population had isolated lung metastasis in 2.1%. This rate is similar to that of other studies, which ranged from 1.5 to 6% [14 –17]. Carlson et al. reviewed 2220 cases of cervical carcinoma and found distant spread in 15% of cases. The lung was the most common site of single organ metastases, followed by supraclavicular lymph nodes, bones, and liver [16].
Survival in uterine cancer patients undergoing pulmonary resection.
PULMONARY RESECTION IN UTERINE AND CERVICAL METASTASES
FIG. 2.
475
Survival in cervix cancer patients undergoing pulmonary resection.
Survival favored uterine cancer patients undergoing lung resection for adenocarcinomas compared to leiomyosarcomas and may be related to the biologic aggressiveness of the latter histology, given its propensity for early hematogenous spread [2]. On the other hand, Levenback et al. [18] reported a more favorable 43% 5-year survival in 45 patients undergoing resection of pulmonary metastases from uterine sarcomas. Most of our uterine cancer patients had one to three lung metastases resected. Resection of three or fewer pulmonary metastasis has been shown to be of positive predictive value in gynecologic [19, 20], as well as other solid tumor lung metastases [12, 19 –24]. We found completeness of resection in our uterine cancer patients to be associated with improved survival. Similarly, the only cervix cancer patient who was incompletely resected did much poorer compared to the others. Complete resection is thought by many to be one of the most important factors necessary for long-term survival [10 –12, 22]. Barter et al. [15] noted greater median times until lung metastasis (DFI) with earlier initial cervical cancer stages, but found initial primary tumor stage to be of prognostic significance only between stage II and stage III patients. In combined gynecological cancer series, Fuller et al. [19] found a prolonged time to initial recurrence of greater than 3 years associated with improved survival. DFI has been considered a predictor of survival in several series of solid tumor pulmonary metastases [12, 21–23]. Mountain et al. [11] reported 5-year survivals of 53% in uterine cancers metastatic to the lung treated by pulmonary resection. Our survival data are nearly identical to that of Bouros et al. [25], who reported a median survival of 25.6 months in patients with uterine metastases treated by pulmo-
nary resection. These results are encouraging given that the majority of patients developing pulmonary metastases from uterine cancer will die in less than 1 year of this ominous disease [25, 26]. Although we had a preponderance of uterine leiomyosarcomas, our survival data are mixed, and factors other than surgery alone may contribute to improved survival. Estrogen and progesterone receptor (ER/PR) status is particularly important to obtain at the time of metastasectomy and is expressed in about one-third of uterine tumors. We recommend routine analysis of ER/PR receptors from pulmonary metastases from uterine cancers to help guide additional treatment with progestational agents. Patients with positive ER/PR receptors have an 80% response rate and average survivals up to 33 months [3]. In contrast, we do not obtain ER/PR receptors in cervix cancer patients because we are not aware of any studies demonstrating efficacy of hormonal treatment in cervical malignancies. Median survival in our cervix cancer patients undergoing pulmonary metastastectomy was 36 months, supporting the role of lung resection in selected patients with cervical cancer metastases. In circumstances where the lung is the only site of recurrence, Imachi et al. also advocate that cervical carcinomas metastatic to lung should be treated by resection [17]. Fiveyear survivals range from 0 to 52% for cervix cancers metastatic to the lung treated by pulmonary resection [10, 11, 20, 27, 28]. In summary, the majority of our patients undergoing lung resection for salvage of uterine metastases tended to have three or fewer lesions and a DFI greater than 1 year. Subset analysis revealed that uterine leiomyosarcomas treated by pulmonary metastasectomy tended to do more poorly compared to uterine
476
ANDERSON ET AL.
adenocarcinomas. Our report conforms to the International Registry of Lung Metastases [12] format so that future series pertaining to these uncommon gynecologic tumors can be more uniformly compared. Cervix cancers with metastases isolated to lung are rare and in our experience are best managed by pulmonary resection.
14. 15.
16.
REFERENCES 1. Greenlee RT, Murray T, Bolden S, Wingo PA. Cancer statistics, 2000. CA Cancer J Clin 2000;50:7–33. 2. Hacker NF. Uterine cancer. In: Berek JS, Hacker NF, editors. Practical gynecologic oncology, 2nd ed. Baltimore: Williams & Williams, 1994: 285–326. 3. Byers LJ, Fowler JM, Twiggs LB. Uterus. In: Abeloff MD, Armitage JO, Lichter AS, Niederhuber JE, editors. Clinical Oncology, 2nd ed. Philadelphia: Churchill Livingstone; 2000:1987–2015.
17. 18.
19.
20.
4. Vermorken JB. The role of chemotherapy in squamous cell carcinoma of the uterine cervix: a review. Int J Gynecol Cancer 1993;3:129 – 42. 5. Martini N, McCormack PM. Evolution of the surgical management of pulmonary metastases. In: McCormack PM, editor. Chest Surg Clin N Am. Philadelphia: Saunders, 1998:13–28. 6. Kaplan, EL and Meier, P. Nonparametric estimation from incomplete observations. J Am Stat Assoc 1958;53:457– 86.
21. 22. 23.
7. Cox DR. Regression models and life-tables. J R Stat Soc B, 1972;34:187– 220. 8. Mann HB, Whitney DR. On a test of whether one of two random variables is stochastically larger than the other. Ann Math Stat 1947;18:50 – 60. 9. Downey R. Surgical treatment of pulmonary metastases. Surg Oncol Clin North Am 1999;8(2):341–54. 10. Abecasis N, Cortez F, Bettencourt A, Costa CS, Orvalho F, De Almeida JMM. Surgical treatment of lung metastases: prognostic factors for longterm survival. J Surg Oncol 1999;72:193– 8. 11. Mountain CF, McMurtrey MJ, Hermes KE. Surgery for pulmonary metastasis: a 20-year experience. Ann Thorac Surg 1984;38:323–30. 12. Pastorino U, Buyse M, Friedel G, Ginsberg RJ, Girard P, Goldstraw P, et al. Long-term results of lung metastasectomy: prognostic analyses based on 5206 cases. J Thorac Cardiovasc Surg 1997;113:37– 49. 13. Ballon SC, Berman ML, Donaldson RC, Growdon WA, Lagasse LD.
24.
25.
26. 27. 28.
Pulmonary metastases of endometrial carcinoma. Gynecol Oncol 1979;7: 56 – 65. Gallousis S. Isolated lung metastases from pelvic malignancies. Gynecol Oncol 1979;7:206 –14. Barter JF, Soong SJ, Hatch KD, Orr JW, Shingleton HM. Diagnosis and treatment of pulmonary metastases from cervical carcinoma. Gynecol Oncol 1990;38:347–51. Carlson V, Delclos L, Fletcher G. Distant metastases in squamous cell carcinoma of the uterine cervix. Radiology 1967;88:961– 6. Imachi M, Tsukamoto, Matsuyama T, Nakano H. Pulmonary metastasis from carcinoma of the uterine cervix. Gynecol Oncol 1989;33:189 –92. Levenback C, Rubin SC, McCormack PM, Hoskins WJ, Atkinson EN, Lewis JL. Resection of pulmonary metastases from uterine sarcomas. Gynecol Oncol 1992;45:202–5. Fuller AF, Scannell JG, Wilkins EW. Pulmonary resection for metastases from gynecologic cancers: Massachusetts General Hospital experience, 1943–1982. Gynecol Oncol 1985;22:174 – 80. Shiromizu K, Kasamatsu T, Takahashi M, Kikuchi A, Yoshinari T, Matsuzawa M. A clinicopathological study of postoperative pulmonary metastasis of uterine cervical carcinomas. J Obstet Gynecol Res 1999;25 (4):245–9. McCormack P. Surgical resection of pulmonary metastases. Semin Surg Oncol 1990;6:297–302. Takita H, Edgerton F, Karakousis C, et al. Surgical management of metastases to the lung. Surg Gynecol Obstet 1981;152:791– 4. Regal AM, Antkowiak JG, Hart T, Takita H. Median sternotomy for metastatic lung lesions: 100 cases. 37th Symposium of the Society of Surgical Oncologists and the Society of Head and Neck Surgeons, May 13–17, 1984, New York: 128. Regnard JF, Cerrina J, Silbert D, et al. Curative surgical treatment of pulmonary metastases. 3rd European conference on clinical oncology, June 16 –20,1985. Stockholm, Sweden, 1985:58. Bouros D, Papadakis K, Siafakas N, Fuller AF Jr. Natural history of patients with pulmonary metastases from uterine cancer. Cancer 1996;78: 441–7. D’Orsi CJ, Bruckman J, Mauch P, Smith EH. AJR 1979;133:719 –22. Cline RE, Young WG. Long-term results following surgical treatment of metastatic pulmonary tumors. Am Surg 1970;36:61– 8. Seki M, Nakagawa K, Tsuchiya S, Matsubara T, Kinoshita I, Went SY, Tsuchiya E. Surgical treatment of pulmonary metastases from uterine cervical cancer: operation method by lung tumor size. J Thorac Cardiovasc Surg 1992;104;876 – 81.