Variations in Etiology and Management of Atrial Fibrillation in a Prospective Registry of 15,400 Emergency Department Patients in 46 Countries: The RE-LY AF Registry Jonas Oldgren, Jeff S. Healey, Michael Ezekowitz, Patrick Commerford, Alvaro Avezum, Prem Pais, Jun Zhu, Petr Jansky, Alben Sigamani, Carlos A. Morillo, Lisheng Liu, Albertino Damasceno, Alex J. Grinvalds, Juliet Nakamya, Paul A. Reilly, Katalin Keltai, Isabelle C. Van Gelder, Afzal Hussein Yusufali, Eiichi Watanabe, Lars Wallentin, Stuart J. Connolly and Salim Yusuf on behalf of the RE-LY Atrial Fibrillation Registry Investigators Circulation. published online January 24, 2014; Circulation is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2014 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7322. Online ISSN: 1524-4539
The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circ.ahajournals.org/content/early/2014/01/24/CIRCULATIONAHA.113.005451
Data Supplement (unedited) at: http://circ.ahajournals.org/content/suppl/2014/01/24/CIRCULATIONAHA.113.005451.DC1.html
Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation is online at: http://circ.ahajournals.org//subscriptions/
Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Variations in Etiology and Management of Atrial Fibrillation in a Prospective Registry of 15,400 Emergency Department Patients in 46 Countries: The RE-LY AF Registry Running title: Oldgren et al.; Atrial Fibrillation - risk factors and management Jonas Oldgren, MD, PhD1; Jeff S. Healey, MD, MSc2; Michael Ezekowitz, MD3; Patrick Commerford, MB, ChB, FCP(SA)4; Alvaro Avezum, MD, PhD5; Prem Pais, MD6; Jun Zhu, MD7; Petr Jansky, MD8; Alben Sigamani, MD6; Carlos A. Morillo, MD2; Lisheng Liu, MD7; Albertino Damasceno, MD, PhD9; Alex Grinvalds, BSc2; Juliet Nakamya, MSc, PhD2; Paul A. Reilly, PhD10; Katalin Keltai, MD, PhD11; Isabelle C. Van Gelder, MD, PhD12; Afzal Hussein Yusufali, MD, MMed13; Eiichi Watanabe, MD, PhD14; Lars Wallentin, MD, PhD1; Stuart J. Connolly, MD2; Salim Yusuf, MD, MBBS, DPhil2 on behalf of the RE-LY Atrial Fibrillation Registry Investigator Investigators rs 1
Uppsala Clinical Research Center and Dept of Medical Sciences, Cardiology, Uppsala University, Uppsala, Sweden; 2Population Health Research Institute, Hamilton, Ontario, Canada; 3Jefferson Medical College, Coll lleg ege, eg e, Wynnewood, Wyn ynn new wood o , PA, and Cardiovascular Research od Reseear arch c Foundation, New York, ch Yorrk, k NY; 4Dept of Medicine Medicine, 5 University Town, Cape Town, South Africa; Univ Un iver e siity ooff Ca Cape pe T own, ow n, C ap pe To Town w , So out u h Af Afri rica caa; Inst Instituto tit itut uto o Dant Dante ntte Pazz Pazzanesse zzan anessee ddee Ca Cardio Cardiologia, i lo logi gia, S Sao a ao Paulo, Brazil; P ulo, B Pa razi ra ziil; 6St. St. John’s John Jo hn’s hn ’s M Medical edic ed ical ic all C College, olle ol lege ege, B Ba Bangalore, angaalo ore, IIndia; ndia nd ia; 7Ca ia Cardiovascular ard r io iova vasscu va ularr IInstitute nsti ns titu ti tute tu te aand nd F Fuwai uwai uw aii Hospital, Beijing, Hospital, Beiji ing, China; Chin na; 8Un University Univ iversi sit ity ty Hospital Hospittal Motol, Mottol tol, Pra Prague, ragu guee, C gu Czech zecch ch Repu Republic; ublic;; 9Eduar ubl Eduardo E d rdo o Mond M Mondlane ondla laanee 100 Univ Un iversity, Ma M puto, Moz M ozamb mb biq que u ; Bo University, Maputo, Mozambique; Boehringer-Ingelheim, B eh hring ngerr-Ing ngellhe heim im m, Ri Ridg Ridgefield, gefieeld d, CT CT; T; 1111Se Semmelweis emmelw mm weiis is University, Univerrsitty, Budapest, Buda Bu dape da pest pe st,, Hungary; st Hung Hu nggary; ary; 12Th Thoraxcenter, T hor orax or a ceent n er,, Univ U University niv ver ersi sity si ty ooff Gr Gron Groningen, onnin inge gen, ge n, U University niive vers rsit rs itty Me M Medical edi diica c l Ce Cent Center nter nt er G Groningen, roni ro niing ngen en,, th en the Netherlands; Nether Ne erla land nds;; 133Du Dubai Duba bai Hospital, Hosppit Ho ital al,, Dubai Du Health Heal He alth th Authority, Aut uthori rity ty y, Du Duba Dubai, bai, i,, U United nite ni ted d Ar Arab ab E Emirates; mira mi rates;; 14De Dept p ooff pt Cardiology, Toyoake, Japan C rd Ca rdio iolo io lo ogy g , Fujita Fuji Fu j taa Health ji Heaalt l h University Univ Un iver iv ersi er s ty School si Sch choo o l of Medicine, Med edic icin ic i e, T oyoa oy oake oa k , Ja ke Japa pan pa n
Address for Correspondence: Jonas Oldgren, MD, PhD Uppsala Clinical Research Center and Department of Medical Sciences, Cardiology Uppsala University S-752 37 Uppsala, Sweden Tel: +46186112765 Fax: +4618515570 E-mail:
[email protected] Journal Subject Codes: Etiology:[5] Arrhythmias, clinical electrophysiology, drugs, Anticoagulants:[184] Coumarins, Treatment:[121] Primary prevention, Treatment:[122] Secondary prevention
1 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Abstract
Background—Atrial fibrillation (AF) is the most common sustained arrhythmia; however little is known about patients in a primary care setting from high, middle and low-income countries. Methods and Results—This prospective registry enrolled patients presenting to an emergency department with AF at 164 sites in 46 countries representing all inhabited continents. Patient characteristics were compared between 9 major geographic regions. Between September 2008 and April 2011, 15,400 patients were enrolled. The average age was 65.9, SD14.8 years, ranging from 57.2, SD18.8 years in Africa, to 70.1, SD13.4 years in North America, p<0.001. prevalence Hypertension was globally the most common risk k factor for AF, ranging in preva vaalenc n e fr from om 41.6% in India to 80.7% in Eastern Europe, p<0.001. Rheumatic heart disease was present in only Africa and on nly 2.2% 2.2% .22% of North Nor orrth American patients, compared ed too 21.5% in Afr frric i a an nd 31.5% in India, p<0.001. use anticoagulation among CHADS p<0 0.0 1. Thee us 0.00 se off ooral raal an anti ticcoag ti coag gul ulat atio ionn am mong patients patien pa en nts ts with witth a C HAD ADS S2 sscore core co re of of 22 wa was as greatest grea gr eate ea test te s in st in North Nort No rthh America Americ Ame icca (65.7%) (6 65. 5 7% 7%)) but but was was only on nly 11.2% 11. % in China, 11.2 Chi hina na,, p<0.001. na p<0. p< 0.00 001. 00 1 The The mean meaan time tim me in me in therapeutic herapeutic range raang ngee was was 62.4% 62.44% in Western 62 Wes este t rn Europe, Eur urop opee, 50 op 50.9 50.9% . % in N .9 North orth or th A America meri me rica ri ca bbut utt oonly nlyy be nl bbetween tween 32% % and 40% in India, China, South-East Asia, and Africa, p<0.001. Conclusions—There is a large global variation in age, risk factors, concomitant diseases and treatment of AF between regions. Improving outcomes globally requires an understanding of this variation and the conduct of research focused on AF associated with different underlying conditions and treatment of AF and predisposing conditions in different socioeconomic settings.
Key words: atrial fibrillation, epidemiology, hypertension, anticoagulation, registry
2 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Introduction Atrial fibrillation (AF) is the most common cardiac arrhythmia1, a leading cause of stroke2 and is associated with increased mortality. Large epidemiologic studies have demonstrated that in most patients, AF is associated with advancing age and underlying cardiovascular disease, particularly hypertension, coronary artery disease and valvular heart disease. However, our current understanding of atrial fibrillation is largely based on data from patients in North America and Europe3-6. Clinical experience and regional cohort studies suggest that other diseases, such as rheumatic heart disease, are more important causes of AF in other regions in the world7,8. However, there are few comparative contemporary data to quantify the relative importance of these hese risk factors in different regions, or to characterize the prevalence of less well-recognized wellell-re r co cogn gniz gn izeed iz ed risk isk factors such as smoking, obesity and sleep apnea9. Ov e the er thee past past as four decades, effective therapies ther errap a ies for atrial fibrillation fib brilllat atio ionn have evolved 10,11; io Over 12-16 16 most mosst st notably, th the he use use off ooral rall anti ra aanticoagulant ntico coaagu co agulaant me medica medications ation ns (O (OAC (OAC) AC)) tto AC o pprevent revvennt sstroke re troke tro oke 12. Ho Howe However; weeveer;
given give gi venn re ve rregional g on gi onal al ddifferences ifffere ferenc nces es inn he health eal alth th ccare arre sy sys systems, stem em ms,, re resource esoourc ourc rcee av availability, vai a laabiili litty, y, expertise exp xpeerti erti tise se aand nd pphysician nd hyysi siccian cian n preferences,, these the hese see therapies the h ra rapi p es are are often ofte of teen applied appl ap plie pl iedd heterogeneously ie hete he teero r ge g ne neou ousl ou slyy17. Th sl The he pu purp purpose rpos rp o e of tthis os hiss st hi sstudy udy was tto o evaluate regional differences in the risk factors of patients with AF, and to describe differences in management.
Methods The RE-LY AF registry enrolled patients who presented to an emergency department (or equivalent acute-care setting) with AF or atrial flutter, either as the primary reason for their visit or as a secondary diagnosis. Consecutive screening of patients was strongly encouraged, although the possibilities for consecutive enrolment were limited due to practical constraints,
3 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
such as the availability of research staff in emergency departments. Centres were also to enrol patients as rapidly as possible and avoid obvious biases in the way patients were identified, such as enrolling only patients who had been admitted to hospital. Where possible, patients with AF were also identified from hospital databases of presenting diagnoses in the emergency department and from systematic review of electrocardiograms conducted in the emergency department. All patients gave written consent for study participation; this was obtained in person by study personnel or via a mail-out information and consent form sent to suitable patients identified from administrative records. A total of 164 sites participated in the AF registry, representing 46 countries from all inhabited nhabited continents (Table 1). Countries were grouped into 9 geographic regions regionns and a d the an the income ncome status of countries defined using the 2011 World Bank definitions18: North America; So out uthh America; Amer Am eric er ica; Western ic Wes e tern Europe (including Australia); Aust stra st r lia); Eastern Eu urope pee, the th Middle East South Europe, (including incclu luding North Nor orth th Africa Afr fric ica and ic an nd Turkey); Turk Tu rkey ey); ey ) Africa; Africaa; India; Indiia; China Chhin na and and South-East SouthSou uth-Ea E st A Ea Asia. sia. si a W Wherever here he reeveer possible, poss po ssib ss ible ib l , registry le reegi gist stry ry y sites sit ites ess inn each each ch region reg egio ionn were io were selected sellec ectted ed to to include in ncl cluudee large larg la r e and rg and small small sma all hospitals; h sp ho spiital it ls; rural rur uraal and and n urban locations; location onns; aacademic cade ca demi de m c an andd co comm community mmun mm unnit ityy se ssettings, ttiing tt ngs, s, aand nd d bboth othh pu ot publ public b icc aand nd pprivate riva ri v te hhospitals. va ospi os pita pi t ls. The study design and protocol was developed by the principal investigators and the study was coordinated and data managed by the Population Health Research Institute at McMaster University in Hamilton, Canada; with additional regional coordination centres in Sao Paulo, Brazil; Beijing, China; Bangalore, India; Prague, Czech Republic; and Seoul, South Korea. Clinical data were collected by interviews with patients, review of medical records and contacts with treating physicians. The diagnosis of all medical conditions including type of AF was based on the clinical record. Persistent AF was defined as episodes which do not terminate spontaneously but do convert with either electrical or pharmacological cardioversion,
4 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
paroxysmal AF as episodes terminating spontaneously, and permanent AF as an episode which does not terminate either spontaneously or with electrical or chemical cardioversion, or where cardioversion has not been attempted. Lone AF was in the data-base defined as AF occurring in individuals less than 60 years old, without concomitant cardiovascular disease (including hypertension), pulmonary disease, hyperthyroidism or recent cardiac surgery. For patients on oral anticoagulation, the three most recent INR values prior to the emergency department visit were collected. There was no biochemical or genetic testing and no central review of imaging studies. The clinical characteristics of patients and their medical treatment for cardiovascular diseases including AF are presented for each region. Continuous variables were compared comp mpar mp ared ed using usi sing ng an analysis of variance and categorical variables using the Chi-square test. An overall p-value wass initially existed wa init in itia it iall ia lly ll y computed comp mput mp uted to test the hypothesis that at nno o difference exi x sted xi d aacross cross all regions with respect significance was esppec e t to eachh patient pattien entt characteristic, ch har arac acte ac teri te rist stic st icc, tthe he sig gniificaanc ance llevel ev vel w as se sett at 00.001. .0 001 01. Each Each h iindividual ndiv nd ivid iv dua uall region egi gion onn was wass then the henn compared co omp mpar ared ed against aga gain ga inst in st the the he other oth ther er regions reegi g onns for fo or each each characteristic cha hara ract cter ct eriisttic for for a further furt fu rthe rt herr understanding understandin ng of o the the existing exiistin ingg global in gllob obal all differences, difffe fere renc re nces nc es,, where es wher wh e e a pre-specified er prepr e sp espec e iffie ec iedd significance sign si gnif gn i iccan if ance ce llevel e el of ev 0.005 was used. The study protocol predefined 10 clinical characteristics for the primary analysis: age, hypertension, diabetes mellitus, coronary artery disease, left ventricular dysfunction, heart failure, valvular heart disease, stroke/TIA, obesity and alcohol use, based on previous studies of risk factors9,19. Only three patients or less had missing data on each of the first eight of these clinical characteristics. Five hundred ninety four patients (3.86%) had missing data for calculation of body mass index, and 1333 (8.66%) of the patients either had missing data or abstained from answering questions about alcohol consumption. We also calculated the CHADS2 stroke risk score20, which assigns 1 point for a history of Congestive heart failure,
5 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Hypertension, Age 75 years or above, or Diabetes mellitus and 2 points for prior Stroke or TIA. The use of oral anticoagulation treatment was further explored in the subgroup of patients admitted to the emergency department with diagnosis of AF prior to the visit and a CHADS2 risk score of 2, which at the time of the study was a general recommendation for oral anticoagulation in all AF treatment guidelines 21. In patients with at least two available INR samples with a maximum of 63 days between consecutive INR values, the degree of INR control was by calculated and presented as the time in therapeutic range as suggested by Rosendaal 22.
Results A total of 15,400 patients with atrial fibrillation (including atrial flutter in 2.3% ooff th thee pa pati tien ti ents en ts) patients) were enrolled at participating emergency departments between September 2008 and April 2011 Taabl blee 22). ). A ). tr al fi tria fibr b illation was the primary rea asonn for visiting th he em mer erge g ncy department in (Table Atrial fibrillation reason the emergency 444.4% 4.44% of cases es. In tot otal a , 27 27.7 .77% off tthe h ppatients he atienntss hadd their theiir first firs fi rsst documented doccum do mentted ment d episode, epi pissode sodee, in 7.6% 7.6 .6% % of of cases. total, 27.7% pa pati tien ti en nts t iitt wa wass un nknow know wn/un n/unce ceerttai ainn if they they hey ha hadd a pr prev ev vio ouss A F di ddiagnosis ag gno nosi s s while si whille a pr whil prio iorr hi io isttor o y off patients unknown/uncertain previous AF prior history AF was found nd d iin n 64 64.6 . % off tthe .6 he ppatients, atie at ieent n s,, ooff tthose hose ho see A F wa w clas assi as siifi fied e aass pe perm rman rm a en an entt in 50.5%, 50. 0 5%, 64.6% AF wass cl classified permanent persistent in 22.6% and paroxysmal in 26.9%. There was a substantial variation in type of AF between the regions, with almost equal distribution between paroxysmal, persistent and permanent AF in Western Europe, while in Africa and the Middle East 81.4% and 71.7%, respectively, of the patients had permanent AF (Table 2). At the conclusion of the emergency department visit, 66.1% of patients were admitted to hospital, 33.7% of patients were discharged home and 0.2% of patients died in the emergency department. The average age of the registry patients was 65.9, standard deviation (SD) 14.8 years, with significantly higher average ages in patients enrolled in North and South America, Western
6 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
and Eastern Europe, China and South East Asia, with the highest age in North America 70.1, SD 13.4 years (Table 2). By comparison, patients in India, the Middle East and Africa were on average approximately 10-12 years younger than the aforementioned six regions. Overall, 4.2% of patients were 35 years old and 28.7% were >75 years old. In total, 52.8% of the patients were males, with the highest proportions of men in Western Europe (61.2%) and North America (58.3%), and the lowest proportions in China (45.5%) and Africa (46.9%). Cardiovascular Conditions Overall, hypertension was the most prevalent AF risk factor and was present in 62.0% of patients. Patients in Eastern Europe had the highest prevalence of hypertension (80.7%), while those Africa, lower hose in Western Europe, India, China, South-East Asia, the Middle East and Af frica ri a, ha hadd a lo lowe w r prevalence, with the lowest prevalence of 41.6% in India (Table 2). Under-reporting of hypertension appeared fewer hype hy pert pe rteensi rt ensi sion o app on pea earred uncommon, as globally fe few wer than 4% off ppatients atieent ntss without a reported history hypertension >160/100 hi tor hist o y of hyp per erttennsio i n ha io hadd a ba bbaseline ase seeliine n bblood lood d ppressure resssure >1 >160 60 0/1 /100 00 ((Table Tablee 22). Tabl ).. Overall, TIA was 13.8% patients. highest rates Over Ov eral er all, l, a hhistory isttory is y ooff st sstroke ro oke or or T IA Aw ass ppresent reesentt iin n 13 13.8 8% off th thee pa ati tien ents en ts.. Th ts Thee hi ighhes estt ra ate tes were seen in China South-East (22.1%), while nC h na ((18.8%) hi 18 8.8 .8%) %) aand nd dS ou uth th-E -Eas -E a t As as Asia ia (2 22. 2 1% %), w hile hi le the he rrate atee of pprior at rior ri or sstroke trok tr o e or TIA ok was substantially lower (7.4%) in India (Table 2). In total, 14.4% of all patients had a history of myocardial infarction, with similar rates in all regions except substantially lower rates in China (7.3%) and Africa (5.5%). A history of heart failure was present in one third of the patients with AF and ranged in prevalence from 17.7% of patients in India to 63.8% of patients in Africa. Among patients with a history of heart failure, the prevalence of systolic left ventricular dysfunction varied from 36.2% in North America to over 60% in Africa, South America and the Middle East, p<0.0001. Valvular heart disease was most common in India (46.7%) and Africa (32.6%), but much less common in Eastern Europe (10.7%) and Western Europe (8.8%) (Table
7 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
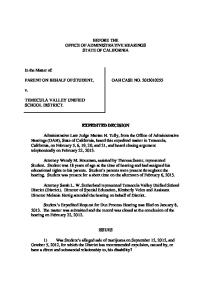
2). Rheumatic heart disease was present in 11.6% of the patients, but only in 1.5% of patients in Western Europe and 2.2% of patients in North America, compared to more than 15% in Africa, the Middle East, China and 31.5% in India (Table 2, Figure 1). In total, 4.7% of the patients had a pacemaker with the highest proportions in North America (8.6%), Western Europe (7.9%) and Eastern Europe (6.9%), but less than 2% of the patients in India and Africa had a pacemaker (Table 2). Recent cardiac surgery and congenital heart disease were uncommon among AF patients worldwide; present in only 1.2% and 2.2% of cases respectively. The average CHADS2 risk score was 1.8 (SD1.4), the highest score was found in Eastern Europe (2.3, SD 1.2) and lower risk in India, China, the Middle East, Africa and Western Europe with the lowest score in India (1.1, SD 1.1) (Table 2). A history of major bleedi bleeding ing ng w was as uncommon (3.8%), with the highest rate in North America (7.9%), and lowest in India (1.5%). Lone Lo n aatrial ne trriaal fi ffibrillation, brillation, i.e. patients below w th the he age of 60 ye years ear a s wi wit without th thout predisposing co conditions, onditions, nd wa was as un unco uncommon, omm mmon on,, re on repr representing pres eseenti es en ing 10 10.7% 0.77% ooff pat patients tieent ntss worl w worldwide orlldw wid de w with ith th h eeven venn lo ve lowe lower w r we proportions South America, Eastern Europe, Africa pr prop opor op orti or t on ti onss in S outh ou th A mer caa, Ea meri East steern st ern Eu Euro ropee, Afr ro A fricaa aand nd IIndia nd dia i (Table (Ta Tabl Ta blle 22). ). Other Conc Concomitant com omit itan antt Co an Cond Conditions dit itio i ns Diabetes mellitus was present in 21.8% of patients with AF, with rates ranging from 15.5% in India to 36.2% in the Middle East; and 11.5% of the patients had chronic obstructive pulmonary disease, ranging from less than 5% in India and Africa to 23.4% in Eastern Europe (Table 2). Obstructive sleep apnea was found in 3.9% of the patients and obesity (BMI 35) in 7.2% of the patients; both conditions were more common in North America, 10.1% and 15.2% of patients respectively, than anywhere else in the world (Table 2). Hyperthyroidism was found in 3.7% of the patients but was more common in Eastern Europe (7.0%) and South East Asia (5.4%). In Africa, more than 8% of AF cases were associated
8 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
with HIV, pericarditis, endomyocardial fibrosis or active tuberculosis; while these four conditions were significantly less common elsewhere (Table 2). Reported alcohol intake was highest in Western Europe and North America. Overall, 17.0% of AF patients had a history of tobacco use and the prevalence was greatest in North America, China, South East Asia and the Middle East and lowest in India (7.5%). Medication in patients with a prior history of AF or other Predisposing Conditions In total, 30.2% received oral anticoagulants, i.e. vitamin K antagonists, ranging from 13.5% in China to 43.5% in North America (Table 3). In patients with prior history of AF and a CHADS2 risk score of 2 but without history of rheumatic fever, 44.9% were treated with an oral anticoagulant at the time of presentation to the emergency department; 65.7% off ppatients atie at ient ntss in nt North America and 63.2% of those in Western Europe (Figure 2). Corresponding rates in other regions egi gion onss varied on vaari ried ed significantly sig ig gnificantly ni from 11.0% to 56%. Among Am patientss w with ithh rh rheu rheumatic e matic heart disease, the China, 50% Africa, over Western Europe he us uusee of OAC AC C rranged ange gedd fr from om 440% 0% % iin n Chi C hina, 50 0% in Af frica, fri ica, too ov verr 885% 5% iin n We West ster ernn Eu er Euro ope pe (Figure results were available OAC Figu Fi gure gu r 22). re ). IINR NR re NR esultts w esul eree av vai aila labble la ble in n 882.1% 2.1% 1% % of of tthe hee ppatients atiient at ient ntss on on O AC ttreatment. reat re a ment at ment nt.. The The Western Europe (67%) proportion ooff INR INR values v lu va ues e between bet etwe ween we en 2.0 2.0 . and and 3.0 3.00 was was highest high hi ghes gh estt in W es e teern E es urop ur opee (6 op (67% 7%)) an 7% aand d lowest in India (35%) (Figure 3). The mean time in therapeutic range, calculated by the Rosendaal method22 for 78.2% of the patients with available INR results, was 62.4% in Western Europe, 50.9% in North America but only between 32% and 40% in India, China, South-East Asia, and Africa (Table 3). Approximately one third of patients with a prior history of AF were treated with aspirin at the time of presentation to the emergency department, ranging from 24.1% in India and 27.2% in Africa to above 40% in North and South America and 48.4% in China (Table 3). Overall, 7.7% of AF patients were on treatment with Clopidogrel, with higher proportions in India
9 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
(14.2%) and the Middle East (10.7%). The most commonly used other pharmacological treatments in patients with prior AF were diuretics, globally in 43.3% of the patients, ranging from one third of patients in China and South East Asia to approximately 50% of the patients in South America, Eastern Europe and Africa (Table 3). In total, almost 30% of the patients received an Angiotensin Converting Enzyme inhibitor (ACE-i), but less than 15% in India and South East Asia, andmore than 50% in Eastern Europe; and approximately 15% had an angiotensin receptor blocker (ARB), with the lowest rates in Africa (6.8%) where treatment with ACE-i was common (Table 3). Beta-blockers were globally prescribed to 41.8% of the patients, ranging from 21.7% in Africa to half of the patients in North America, Western and Eastern Europe. A quarter of the patients tss had had a ddigoxin, igox ig oxiin, ox i n, ranging anging from 12.7% in Western Europe to more than one third of patients in India and Africa, and an nd in total tot otal tal 8.2% 8.2% % had ha verapamil or diltiazem, with wiith th only only 2.0% in Africa A rica Af caa up up to 18.5% in North America (Table 3). Off th specific amiodarone was most common with Amer Am e ica (Tabl blee 3) ). O thee sp pecif ecific ic aantiarrhythmic nttiaarrhyyth hmicc ddrugs, rug uggs, am mio ioddarone w as m as ost co ost ommon mmonn w ih it 8.7% with North America, Western 8. .7% gglobally, loba lo baall lly, y, aalthough lthhoug houg ughh wi w th h a llarge argge vvariation ar ari riat atio at ionn fr io ffrom om 5% % or lless esss iin n No Nort rtth Am Amer e ic er i a, W esste tern r rn Middle East and Africa South America Eastern Europe. other Europe, the Mi Midd d le E dd a t an as nd Af Afri r ca tto ri o ov over er 115% 5% iin n So S uthh Am ut Amer eric er i a an ic andd Ea East ster st errn Eu Euro rope ro p . All othe er antiarrhythmics, e.g. flecainide, propafenone, sotalol, disopyramide, dofetilide, and quinidine, were globally prescribed in 2% or less of the patients albeit with some regional variations, most prominent with higher rates of propafenone in Eastern Europe (4.4%) and China (3.9%) and sotalol in Eastern Europe (3.4%) (Table 3). Overall, less than one third of the patients had lipid lowering drugs, most commonly statins (26.3%), ranging from only 6.2% in Africa to 42.2% in North America (Table 3). The proportion of patients with a history of hypertension who did not receive antihypertensive therapy was only 3.7% in North America, but was over 10% in South-East Asia,
10 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Africa and Eastern Europe (Table 3). Among patients with a history of hypertension, the baseline systolic blood pressure was highest in Africa (142.2, SD 29.0 mmHg), Eastern Europe (140.5, SD 22.7 mmHg) and China (140.0, SD 23.2 mmHg). Similarly, the prevalence of left ventricular hypertrophy among patients with hypertension was highest in Eastern Europe (46.2%) and Africa (38.1%) (Table 2). The majority (51.9%) of heart failure patients received treatment with ACE-i or ARB, ranging from more than two thirds of patients in South America to only one third in India and China, while overall 45.6% of patients received beta-blockers for the treatment of heart failure, ranging from almost two thirds in North America and Western Europe to only one fifth of patients in Africa (Table 3). Exploration of Regional Differences in Patient Age Given significant rheumatic Give Gi venn th ve thee si sig gniffic icaant an regional differences in thee pr pprevalence evalence of rheu eumaati eu ticc and infectious diseases and substantially with an nd th tthat at patients patient ntss with with th h these theese conditions con ondi diti t ons ti ons tend teend to be su ubsttan tantia ntiaallly yyounger ounge ungerr tthan han n tthose hosee w hose ithh it cardiovascular and ca ard rdio iova io v sc va scul ular ul ar disease diseease easee and and hypertension, hyp y er erte tennsio te nsio on, the the bbaseline aseeliine ddemographics emoogra em ogra raph ph hiccs an nd pr pprevalence eval ev alen al en nce off cardiovascular each with cardiovascullar cconditions on ndi d tiion ons we were r rre-analyzed e an eanallyz y ed ffor or ea ach rregion, eg gio ion, n, after aft fter er excluding excl clud udin ud ingg patients in paatiien ents ts w ith rheumatic heart disease, HIV, active tuberculosis, endomyocardial fibrosis, Chagas disease and pericarditis (Supplemental Table 1). Exclusion of these patients resulted in more similar distribution of age across regions, but patients in India, the Middle East and Africa were still at least seven years younger.
Discussion This is one of the largest prospective registry studies of AF and the first global registry to include unselected patients in the emergency department, with a significant numbers of individuals from
11 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
middle and low income countries, and representing all inhabited continents. It demonstrates a wide regional variation in the risk factors, concomitant diseases and treatment of AF. Patients with AF from middle and low income countries are significantly younger than those from highincome countries, the diseases associated with their AF are quite different and these patients are less likely to be managed according to published AF guidelines 21. Despite large regional variations in prevalence, hypertension is the most common risk factor for AF globally. Thus to prevent AF, more effective strategies to diagnose, treat and control hypertension need to be implemented 23. This need is greatest in Eastern Europe and Africa, where hypertension is most likely to be untreated and poorly controlled and where approximately 40% of hypertensive patients have evidence of left ventricular hyp hypertrophy; ypperrtr t op ophy hy;; a hy marker of prolonged uncontrolled hypertension and of poor outcomes. As well, approximately 60 60% 0% of iindividuals ndiv nd iviidua iv uaals iin n these two regions had a history hiisto story of heart fail failure ilur u e an and/or nd/or d/ systolic left vventricular enntri ntr cular dysfunction, dy ysffun unct ctio ion, io n, w which hich m hich might ighht ig ht be be secondary seccondarry to their thei th eirr predisposing prred ediispposi posiing con conditions on ndi diti tion on ns fo forr AF AF,, typically hypertension these ypi pica caall l y hy hype pert rteenssion sionn aand nd vvalvular a vuula al larr hheart eart disease. dis isea eaase s . Earlier Earllieer identification Earl iden id nti t fi fica caati tion onn and and treatment treeat a me mennt of of th thes esse risk isk factors in in the the community comm co mmun mm nit i y could co oul u d lead l ad to le to improved impr im prov pr oved ov ed d patients pat atie ieent ntss outcomes outc ou t om omes es and and reduced red educ uced uc ed aacute-care cute-care costs24. Rheumatic heart disease remains an important cause of AF in Africa, China, the Middle East and particularly in India, where it is present in nearly one-third of patients with AF. In fact, the true prevalence in these regions is likely higher, as this registry did not include routine echocardiography, which is sensitive for the diagnosis of rheumatic heart disease 25. Although rheumatic heart disease is strongly associated with lower socioeconomic status 26, low-cost strategies to prevent the development and recurrence of rheumatic heart disease could have a great impact on preventing the development of AF and its complications27-29. The average age of
12 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
patients with AF and rheumatic heart disease in this registry was 52 (SD 22) years and 66.2% were women, many of whom were of child-bearing potential. Thus, the consequences of AFrelated stroke are great in this cohort, but so are the challenges for stroke prevention. Although patients with rheumatic heart disease are one of the highest-risk groups for stroke, virtually all research into stroke risk stratification schemes and randomized trials of anticoagulant therapy have excluded patients with rheumatic heart disease or severe heart valve disorders 12,14-16,30. Stroke prevention therapies, including the new oral anticoagulants should be evaluated in patients with rheumatic heart disease. To be feasible and relevant, these studies should be conducted in the regions where rheumatic AF is most prevalent. 2,7,31,32 2,7,31 ,31,,32 ,31 orlldw dwid id de 2,7 . Atrial fibrillation remains a major cause off death, stroke and disability wo worldwide
Over the last 15 years, many important clinical studies have improved our ability to prevent the morbidity morb mo rbid rb idit id ityy an it aand d mo mor mortality rta ity of AF 10,12,14-16,33. The be rtal bene benefits neefits of this res research sea e rcch have ha been realized largely arg gel e y by ind individuals div ivid i uals id uals inn hi high high-income gh--inco gh inco ome me ccountries, ounttriees, ffor orr wh whom hom om tthe he rresearch he esea earc rchh was was ta targeted. arg rget eted et ed d. Th T Thee appropriate patients with non-valvular AF additional appr ap prop pr opri op riat atee use usee of us of oral ora rall anticoagulation antico anti oagu gula lati la tion ti onn inn pa patien ents en tss w ithh no non n-va n-va valv l ul lv u ar A F an andd ad addi dittio tional all rrisk ik is 12,14,16 12,14 14,16 14 16 factors can reduce redu re duce du cee the the h rate rat a e of stroke sttro roke ke by by two two thirds thir th irds ir dss or or more mo ore 12 . Ho Howe However, weve we ver, ve r, ooral rall an ra anti anticoagulation tico ti c agulation
was in the present study population prescribed for only 58% of patients worldwide with a prior history of non-rheumatic AF and a CHADS2 score of 2. Use of oral anticoagulants in these AF patients at risk for stroke was 40% or less in Eastern Europe, India and Africa where access to INR testing and follow-up are limited, and was only11% in China where physicians have concerns about the rate of warfarin-related intra-cranial hemorrhage and disagreement exists as to the appropriate therapeutic ranges of INR 34,35. INR control was also particularly poor in these regions, but only approached desired levels 36 in Western Europe. Low cost generic strategies may be considered to overcome these hurdles in low- and middle income countries, using non-
13 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
physician health workers especially at local community centers or even in people’s homes, where INR:s can be checked once a month with point of care devices purchased in bulk by governments and provided to each clinic. The advent of novel oral anticoagulants 14,16 may help to overcome some of these barriers; however, their current high costs may make these novel drugs affordable for only a select group of individuals who are either wealthy or have private health insurance. For the majority of patients in these regions, strategies to diagnose hypertension early and improve its control, improve the management of warfarin 37 or the use of combination antiplatelet medications 38. Although the combination of aspirin and clopidogrel is less effective than oral anticoagulants, this treatment does not require regular monitoring and may be affordable, thereby hereby a wider use may not be ideal but better than no stroke prevention treatme treatment. meent nt.. The region-specific differences identified in this registry may also give opportunities to improve mpr prov ovee care, ov care ca r , which re whhic ichh should lead to increased physician phy hysiician and patient hy patieent n awareness awa warreness wa re through educational ed ducational uc st strategies, tra ratteg tegies es, ma mana management nage geme ge ment nt aand nd preve nd prevention ventio ve on str strategies rategi rat tegiiess aand nd uultimately nd ltim lt imaatel im elyy to to cchanges h nge ha nges iin n pub ppublic ublic policy middle-income poli po licy li cy in in order orrde derr too maximize max xim miz ize benefit b ne be nefi fitt in low fi low and andd m iddle-in idd e-in nco come me ccountries. ount ou ntri nt riees.. Government Gooveern rnme ment me nt level lev ev vel policy changes chang ngges are aree needed neeede d d to improve imp mpro r ve ro v hygiene hyg ygie ieene and and access acc c ess s to to affordable affo af ford fo rd dab able le health hea ealt l h care lt care to to control thee growing incidence of rheumatic heart disease. Strategies may also include screening for rheumatic heart disease and systems of care to include routine electrocardiograms once in five years in elderly or patients with specific risk factors for AF, such as hypertension, vascular disease or valve disease. Limitations and Strengths As this registry did not include patients without AF, it cannot provide a direct measure of AF prevalence in the emergency department or determine the population-attributable risk for the various AF risk factors. However; the latter have been well-documented in earlier studies 9,39 and
14 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
the current study’s focus is on comparing the relative prevalence of established risk factors between global regions. The current registry did not include consecutive patients; however, patient characteristics are similar to smaller regional registries that did 7,8. Although this registry is not population-based, its recruitment of primary care patients from emergency departments avoids many of the biases of other multinational registries which enrolled patients from specialist physicians’ offices 40. Finally, echocardiography was not performed as part of the protocol and was not uniformly done throughout the world, thus the ascertainment of left ventricular hypertrophy and valvular disease may have differed between regions. However; the regions with the highest reported prevalence of these two conditions were among those with the lowest use of cardiac technology 41, including echocardiography, thus the regional differencess oobserved bsserrve vedd in tthis his registry egistry were if anything an under-estimate of the disparity. Despite Desp De spiite sp it these th hese es limitations, the RE-LY AF F registry r gistry has several re sever eral strengths, er str treengths, en including its large size izee aand nd its bro broad road ad gglobal lo oba b l re representation epr pres esen enta t ti ta t onn ooff co countries, ountriies, in including ncluddinng nclu ng m many any lo low w an and nd mi midd middle-income ddle dd le-i le -inc inc ncom omee om countries, co ountr untr trie i s,, many ie many any off which whicch ch have hav ve never neve ne verr been ve been included inc nclu lude lu deed inn prior pri rioor or registries reg egiistrrie iess or or clinical cli linniccal a trials tri riaals off ppatients attieent ns with AF.
Conclusions There is wide regional variation in the age, the presence of stroke risk factors, concomitant diseases and in the treatment of patients with AF. Improving outcomes globally requires an understanding of this variation, and the conduct of research focused on AF associated with different underlying conditions and of treatment of AF and predisposing conditions in different socioeconomic settings.
15 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Funding Sources: The RE-LY AF Registry was funded by an unconditional grant from Boehringer-Ingelheim.
Conflict of Interest Disclosures: JO reports institutional research grants from BoehringerIngelheim. JH reports research grants from Boehringer-Ingelheim and Bristol-Meyers-Squibb, and is supported by a personnel award from the Heart and Stroke Foundation, Ontario Provincial office (MC 7450). EW reports lecture fees from Bayer Healthcare and Boehringer-Ingelheim.
References: 1. Furberg CD, Psaty BM, Manolio TA. The prevalence of atrial fibrillation in elderly subjects. Am J Cardiol. 1994;74:236-241. 2. Wolf PA, Abbot RD, Kannel WB. Atrial fibrillation as an independent risk factor fac acto torr fo to forr st stro roke ro ke: ke stroke: The Framingham Study. Stroke. 1991;22:983-988. 3. Kannel WB, Abbot RD, Savage DD, McNamara PM. Epidemiologic features of chronic atrial fibrillation. fibr ril illa lati la tion ti on.. T on The hee F Framingham ramingham Study. N Engl J M ra Med. ed. 1982;306:1018-10 ed 1982;306:1018-1022. 10022 22. 4.. Kannel Kan a nel WB, WB B, Wolf Wolff PA, PA, Benjamin Ben nja jami minn EJ. mi EJ Prevalence, Prev Pr eval ev a en al nce,, incidence, in nci cide denc de nce, nc e, prognosis, pro rogn gnos gn osis os is, and is an nd predisposing pred pr edis ed i po is posi sing si ng conditions cco onditions nd for at atrial triaal fi fibr fibrillation: briillati tiion: Po Population-based opu pullation--baased d eestimates. stim mat ates es. Am J Car es Cardiol. rdi diol ol. 199 1998;82:2N-9N. 998; 8 82:2 82:2NN-9N 9N.. 5 Krahn 5. Kra rahn hn AD. AD. The The natural nat atur ural ur al history hissto tory ry of of atrial atri at rial ri al fibrillation: fib ibri rill ri l at ll atio ionn: Incidence, io Inc ncid iden id ence en ce, risk risk factors fac acto t rs and to and prognosis pro rogn gnos gn osis os is iin n th tthee Mainitoba Med. 1995;98:476-484. Main Ma init in itob it obaa Follow-up ob Foll Fo llow ll ow-u -up up Study. Stud St udyy. Am J M ud ed. 19 ed 1995 95;9 95 ;98: ;9 8:47 8: 4766-48 47 6-48 4844. 6. Nieuwlaat R, Capucci A, Camm AJ, Olsson SB, Andresen D, Davies DW, Cobbe S, Breithardt G, Le Heuzey JY, Prins MH, Lévy S, Crijns HJ. Atrial fibrillation management: the Euro Heart Survey on Atrial Fibrillation. Eur Heart J. 2005;26:2422-2434. 7. Ntep-Gweth M, Zimmermann M, Meiltz A, Kingue S, Ndobo P, Bloch A. Atrial fibrillation in Africa: clinical characteristics, prognosis and adherence to guidelines in Cameroon. Europace. 2010;12:482-487. 8. Zubaid M, Rashed WA, Alsheikh-Ali AA, Al Mahmeed W, Shehab A, Sulaiman K, AlZakwani I, Alqudaimi A, Asaad N, Amin H. Gulf survey of atrial fibrillation events (Gulf SAFE): Design and baseline characteristics of patients with atrial fibrillation in the Arab Middle East. Circ Cardiovasc Qual Outcomes. 2011;4:477-482. 9. Huxley RR, Lopez FL, Folsom Ar, Agarwal SK, Loehr LR, Soliman EZ, Maclehose R, Konety S, Alonso A. Absolute and attributable risks of atrial fibrillation in relation to optimal and borderline risk factors. Circulation. 2011;123:1501-1508.
16 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
10. Wyse DG, Waldo AL, DiMarco JP, Domanski MJ, Rosenberg Y, Schron EB, Kellen JC, Greene HL, Mickel MC, Dalquist JE, Corley SD. A comparison of rate control and rhythm control in patients with atrial fibrillation. N Engl J Med. 2002;347:1825-1833. 11. Nair GM, Nery PB, Divakaramenon S, Healey JS, Connolly SJ, Morillo CA. A systematic review of randomized trials comparing radiofrequency ablation with antiarrhythmic medications in patients with atrial fibrillation. J Cardiovasc Electrophysiol. 2009;20:138-144. 12. Hart RG, Pearce LA, Aquilar MI. Meta-analysis: Anti-thrombotic therapy to prevent stroke in patients who have nonvalvular atrial fibrillation. Ann Intern Med. 2007;146:857-867. 13. Connolly SJ, Eikelboom J, Joyner C, Diener HC, Hart R, Golitsyn S, Flaker G, Avezum A, Hohnloser SH, Diaz R, Talajic M, Zhu J, Pais P, Budaj A, Parkhomenko A, Jansky P, Commerford P, Tan RS, Sim KH, Lewis BS, Van Mieghem W, Lip GY, Kim JH, Lanas-Zanetti F, Gonzalez-Hermosillo A, Dans AL, Munawar M, O'Donnell M, Lawrence J, Lewis G, Afzal R, Yusuf S. Apixaban in patients with atrial fibrillation. N Engl J Med. 2011;364:806-817. Al-Khalidi HR, 14. Granger CB, Alexander JH, McMurrary JJ, Lopes RD, Hylek EM, Hanna M, Al Al-K - ha -K hali lidi di H R Flaker Garcia Ansell J, Atar D, Avezum A, Bahit MC, Diaz R, Easton JD, Ezekowitz JA, Flake keer G, G G arci ar ciaa D, ci Geraldes M, Gersh BJ, Golitsyn S, Goto S, Hermosillo AG, Hohnloser SH, Horowitz Horow ow wit itzz J, J Mohan Moh ohan an P, Jansky P, Lewis BS, Lopez-Sendon JL, Pais P, Parkhomenko A, Verheugt FW, Zhu J, Wallentin L. Apixaban Api p xaban versus warfarin in patients with atrial fibrillation. N Engl J Med. 2011;365:981-992. 20 011 11;3 ;365 ;3 65:9 65 :981 :9 81-9 81 992 92. Patel Mahaffey W,, Ga Pan Singer Hacke W,, B Breithardt Halperin 115. 5. P atel MR, M ahhaff haff ffey ey yW Garg rg JJ,, Pa an G, S ingeer DE DE,, Hack H ack c eW reit re i hard it dt G, G, H allpe p ri r n JL JL,, Hankey Piccini JP, Becker RC,, Ne Nessel CC, Paolini Berkowitz KA, Califf RM. H annkey nk GJ, P icccin cini JP P, B eccker ker RC R Ness sel C C, Pa aolin olinii JF JF, Be Berk kow witz SD SD,, Fo Foxx KA A, Ca alifff R M. Rivaroxaban Engl Med. Ri ivaro varo roxa xaba baan versus verrsuus ve us warfarin warrfa fari r n in nonvalvular non onva valv l ul lv ular ar atrial atr tria iall fibrillation. fibrril fibr illa lati la tion ti on.. N En on ngl g JM ed d. 22011;365:883-891. 011; 01 1;33655:88831; 883-89 91. 1 16. Connolly SJ, Ezekowitz MD, Yusuf S,, Ei Eikelboom Oldgren Parekh A,, Po Pogue ly yS J, E zeko ze k wi ko w tz M D Y D, u uf S us Eike kelb ke lb boo oom m J, O ldgr ld gren gr en JJ,, Pa Pare rekh re kh A Pogu guee J, Reilly gu PA, Themeles E, Va Varrone Wang S, A Alings M, X Xavier D, Z Zhu R, Le Lewis BS, Da Darius H, PA Th Them emel eles es E Varr rron onee JJ, W angg S an ling li ngss M avie av ierr D hu JJ, Di Diaz az R Lewi wiss BS Dari rius us H Diener HC, Joyner CD, Wallentin L. Dabigatran versus warfarin in patients with atrial fibrillation. N Engl J Med. 2009;361:1139-1151. 17. Gao Q, Fu X, Wei JW, Chen X, Huang J, Anderson CS, Wong KS. Use of oral anticoagulation among stroke patients with atrial fibrillation in China. Int J Stroke. 2013;8:150154. 18. World Bank list of economies 2011. http://wdronline.worldbank.org/worldbank/a/incomelevel. 19. Conen D, Tedrow UB, Cook NR, Moorthy MV, Buring JE, Albert CM. Alcohol consumption and risk of incident atrial fibrillation in women. JAMA. 2008;300:2489-2496. 20. Gage BF, Waterman AD, Shannon W, Boechler M, Rich MW, Radford MJ. Validation of clinical classification schemes for predicting stroke: results from the National Registry of Atrial Fibrillation. JAMA. 2001;285:2864-2870.
17 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
21. Fuster V, Rydén LE, Cannom DS, Crijns HJ, Curtis AB, Ellenbogen KA, Halperin JL, Le Heuzey JY, Kay GN, Lowe JE, Olsson SB, Prystowsky EN, Tamargo JL, Wann S, Smith SC Jr, Jacobs AK, Adams CD, Anderson JL, Antman EM, Hunt SA, Nishimura R, Ornato JP, Page RL, Riegel B, Priori SG, Blanc JJ, Budaj A, Camm AJ, Dean V, Deckers JW, Despres C, Dickstein K, Lekakis J, McGregor K, Metra M, Morais J, Osterspey A, Zamorano JL. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation - executive summary. J Am Coll Cardiol. 2006;48:854-906. 22. Rosendaal FR, Cannegieter SC, van der Meer FJ, Briet E. A method to determine the optimal intensity of oral anticoagulation therapy. Thromb Haemost. 1993;69:412-417. 23. Quinn RR, Hemmelgarn BR, Padwal RS, Myers MG, Cloutier L, Bolli P, McKay DW, Khan NA, Hill MD, Mahon J, Hackam DG, Grover S, Wilson T, Penner B, Burgess E, McAlister FA, Lamarre-Cliche M, McLean D, Schiffrin EL, Honos G, Mann K, Tremblay G, Milot A, Chockalingam A, Rabkin SW, Dawes M, Touyz RM, Burns KD, Ruzicka M, Campbell NR, Vallée M, Prasad GV, Lebel M, Tobe SW. The 2010 Canadian Hypertension Education Program recommendations for the management of hypertension. Can J Cardiol. 2010;26:241-248. 24. O'Reilly DJ, Hopkins RB, Healey JS, Dorian P, Sauriol L, Tarride JE, Burkee N N,, Go Goeree RA. Goer eree ree R A. The burden of atrial fibrillation on the hospital sector in Canada. Can J Cardiol. 2013;29:229201 0133;29 3;29 29:2 :229 :2 29-29 235. 25. R,, Wi Wilson heart disease 255. We Webb bb R Wils lsoon ls on NJ, Lennon D. Prevalence of of rrheumatic heumatic hea art dis sea easse detected by echocardiographic screening. Med. ecchoocardiogr grrap a hiic sc scre reeen enin ing. in g. N En Engl g JM gl ed.. 22007;357:470-476. ed 0077;3357::47 00 4700 47 04 6.. 26. S,, Ro A,, Sethh S S,, K Krishnan Misra Kalaivani M,, B Bhargava B,, 266. Saxena Saxena A, A, Ramakrishnan Raamakkrisshnnan S Royy A riish shna nann A, na A M issraa P, Ka Kala aiva ivani ani M harrgav va B Flather MD, Poole-Wilson PP. Prevalence outcome rheumatic Flat Fl athe at herr MD he D, Poo P oolee-W e-Wilsson P P P P. reva re vale leencce aand ndd ou utccom me of ssubclinical ubcl ub cllin nic ical al rh heum heum mat atic ic hheart eartt ddisease i eaasee iin is n India: Rheumatic Study. ndi dia: a: tthe he R heeum umat atic ic S tudy dy. Heart. Hearrt. He t 2011;97:2018-2022. 2011 1;9 ;97: 7:20 2018 18-202 022. 2 27. Marijon E, M Mirabel M, Ce Celermajer DS, X. R Rheumatic Lancet. 27 Ma Mari rijo jonn E irab ir abel el M Cele lerm rmaj ajer er D S aand nd JJouven ouve ou venn X heum he umat atic ic hheart eart ea rt disease. dis isea ease se La Lanc ncet et 2012;379:953-964. 28. Viali S, Saena P, Futi V. Rheumatic fever programme in Samoa. N Z Med J. 2011;124:26-35. 29. Carapetis JR, Zuhlke LJ. Global research priorities in rheumatic fever and rheumatic heart disease. Ann Pediatr Cardiol. 2011;4:4-12. 30. Gage BF, Van Walraven C, Pearce L, Hart RG, Koudstaal PJ, Boode BS, Petersen P. Selecting patients with atrial fibrillation for anticoagulation: Stroke risk stratification in patients taking aspirin. Circulation. 2004;110:2287-2292. 31. Lamassa M, Di Carlo A, Pracucci G, Basile AM, Trefoloni G, Vanni P, Spolveri S, Baruffi MC, Landini G, Ghetti A, Wolfe CD, Inzitari D. Characteristics, outcome, and care of stroke associated with atrial fibrillation in Europe: data from a multicenter multinational, hospital-based registry. Stroke. 2001;32:392-338.
18 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
32. Benjamin EJ, Wolf PA, D'Agostino Sr.RB, Silbershatz H, Kannel WB, Levy D. Impact of atrial fibrillation on the risk of death: the Framingham Heart Study. Circulation. 1998;98:946952. 33. Roy D, Talajic M, Nattel S, Wyse DG, Dorian P, Lee KL, Bourassa MG, Arnold JM, Buxton AE, Camm AJ, Connolly SJ, Dubuc M, Ducharme A, Guerra PG, Hohnloser SH, Lambert J, Le Heuzey JY, O'Hara G, Pedersen OD, Rouleau JL, Singh BN, Stevenson LW, Stevenson WG, Thibault B, Waldo AL. Rhythm control versus rate control for atrial fibrillation and heart failure. N Engl J Med. 2008;358:2667-2677. 34. Shen A Y-J, Yao JF, Brar SS, Jorgensen MB. Racial/Ethnic differences in the risk of intracranial hemorrhage among patients with atrial fibrillation. J Am Coll Cardiol. 2007;50:309315. 35. You JH, Chan FW, Wong RS, Cheng G. Is INR between 2.0 and 3.0 the optimal level for Chinese patients on warfarin therapy for moderate-intensity anticoagulation? Br J Clin Pharmacol. 2005;59:582-587. 36. Connolly SJ, Pogue J, Eikelboom J, Flaker G, Commerford P, Franzosi MG MG, Healey G, He Heal aley ey JJS, S, Yusuf S. Benefit of oral anticoagulant over antiplatelet therapy inn atrial fibrillation fibrillatiion n depends dep pen ends ds oon n the he quality of international normalized ratio control achieved by centres and countries as measured byy time in therapeutic range. Circulation. 2008;118:2029-2037 2008;118:2029-2037. 37. 37. T,, Wi Wilczynski NL, Haynes 37 7. Nieuwlaat Ni Nieuwl laaat R,, Connolly Con onno noll no llly SJ, SJ, Mackay Mack Ma ckay ay y JA, JA,, Weise-Kelly Wei eisee-K Kellly L, Navarro Nav varro arro T W lcczy zyns nski ns ki N L, H ayne ay n s ne RB. Computerized decision systems for therapeutic monitoring dosing; RB.. Computer eriz ized ed d cclinical lini li nica call de ca dec cision cisi on ssupport upportt sy upp ystem em ms fo or th the eraape apeutic dr ddrug ug m onit on itor orrin ingg aand nd do dosi sinng; A decision-maker-researcher deecision-m mak a er--resea earrche heer partnership partneers part r hipp systematic syssteemaaticc review. rev evie iew ie w. Implementation Imppleemen nta ati tioon SScience. c en ci ncee. 22011;6:90. 011;66:990. 38. AC ACTIVE ACTI TIVE VE IInvestigators, nvessti nv tiga g tors rs, Connolly Conn Co nnol olly SJ, J Pogue Pog ogue ue J Hart Har artt RG, RG Hohnloser Hohnnlo Ho lose serr SH, SH H, Pfeffer Pfef Pf effe fer M, Chrolaviciuss S S,, Yu Yusuf Effect aspirin patients with atrial Yusu suff S. su S E ffec ff e t of cclopidogrel l pi lo pido dogr do grel gr el aadded dded dd ed tto o as aspi piri pi r n in pa ri pati tien ti ents en ts w ithh at it atri rial ri al ffibrillation. ibrillation.. N En Med. Engl gl J M ed 2009;30:2066-2078. 200 009; 9;30 30:2 :206 0666-20 2078 78 39. Benjamin EJ. Independent risk factors for atrial fibrillation in a population-based cohort. The Framingham Heart Study. JAMA. 1994;271:840-844. 40. Le Heuzey JY, Breithardt G, Camm J, Crijns H, Dorian P, Kowey PR, Merioua I, Prystowsky EN, Schwartz PJ, Torp-Pedersen C, Weintraub W. The RECORDAF study: Design, baseline data and profile of patients according to chosen treatment strategy for atrial fibrillation. Am J Cardiol. 2010;105:687-693. 41. Millar RN, Mayosi BM. Utlization of implantable defibrillators in Africa. Card Electrophysiol Rev. 2003;7:14-16.
19 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Table 1. Participating Countries by Region and Income Status Region (number of centres)
Number of List of Countries (number of centres) Countries
World Bank Income Group (number of countries)
North America (19)
2
Canada (7), United States (12)
Upper-Income (2)
South America (23)
6
Argentina (3), Brazil (13), Chile (3), Colombia (2), Ecuador (1), Venezuela (1)
Middle-Income (6)
Western Europe (19)
10
Australia (1), Austria (1), Denmark (1), Germany (4), Ireland (1), ( ), Italyy (2), ( ), the Netherlands (2), ( ), Spain p (1), ( ), Sweden (4), United Kingdom (2)
Upper-Income (10)
Eastern Europe (22)
8
Bulgaria (2), Czech Republic (8), Hungary (3), Latvia (3), Poland (1), Russia (1), Slovakia (2), Ukraine (2)
Upper-Income Uppe Up ppe perr In Inco come co me ((4) 4 Middle-Income M dd Mi ddle dle l -Inc I com me ((4)
India (22) 2)
1
India (22)
Middle-Income ((1)
China (20) 0)
1
China (20)
Middle-Income ((1)
South-East ast Asia Asiia (11) (11))
4
Japan (1), Korea (7), Singapore (2), Thailandd ((1) Singapore a 1)
(3) Upper-Income (3 Middle-Income Midd Mi ddle le-I -Inc ncom ome ((1)
Middle East Eastt (8) ( ) (8
5
Egypt Egyp Eg ypt (2), yp ( ), Iran (2 Ira ran (1), 1 Saudi S udi Sa d Arabia A abia Ar bia (1), (1) 1),, Turkey Turk Tu urkey ey (1), (1) 1), United United te Arab A ab Ar b Emirates Emi mira r te tes (3) 3)
Upper-Income Upp rUppe r-In I co In come m (2 (2) Middle-Income M dd Mi d le le-Inccome m ((3)
Africa (20) 20) 20 0)
9
Cameroon (2), Kenya Mozambique Nigeria (7), C mero Ca meero r onn (2) 2 , Ke 2) K nya ya (1 (1), ) M ozam oz ambi mbiqu q e (2 ((2), ), N ), ig ger e iaa (7) 7, 7) Senegal S ne Se nega gall (1), (1)), (1 ), South South h Africa Afr f ic icaa (3), (3), ) Sudan Sud udan a (1), an (1) 1),, Tanzania Tanz Ta nzan nz ania an iaa (1), (1) 1),, Uganda Uggan anda (1), (1)), Zambia Zamb Za mbia ia (1) (1))
Middle-Income M dd Mi d le le-Inccome m ((5) Lower-Income Lo owe werr In rInco come co me ((4) 4
Over all
46 4
Upper-Income (21) Up (22 Middle-Income Midd Mi ddle le Inc ncom omee (2 ((21) 2 Lower-Income (4)
20 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Table 2. Cardiovascular and other Concomitant Conditions and Risk Factors North South Western Eastern India China SouthEast Middle Africa America America Europe Europe Asia East Number of Patients 15400 1817 1134 1983 2542 2536 2023 1341 887 1137 † Age, years (SD) 65.9 (14.8) 70.1* 68.3* 69.4* 69.3* 57.9* 68.4* 69.5* 58.6* 57.2* (13.4) (13.1) (12.1) (11.0) (15.8) (13.2) (13.2) (15.6) (18.8) Age, IQR 57-77 62-80 60-78 62-78 62-78 46-70 60-78 61-79 48-71 46-71 † Male 52.8 56.0 55.4 56.4 58.3* 61.2* 49.8* 49.7* 45.5* 46.9* 64.6 70.4 65.9 69.8 76.5 42.4 80.6 770.5 0.55 0. 55.8 55 .8 39.3 Prior atrial rial fibrillation † Paroxysmal 26.9 46.3 26.7 14.5* 36.7* 17.6* 20.5* 34.2 34 .2** .2 20.8 20 .8** .8 34.2* 20.8* 8.9* Persistent† 22.6 13.0 31.9* 28.7* 30.0* 32.9* 18.5* 13.3 13 13.3* 3* 77.5* .5* 9.6* † Permanent 50.5 40.4 53.4 52.3 46.6 52.5 81.4* 34.6* 54.8* 71.7* Cardiovascular vascular Conditions Hypertension nsion† 62.0 559.9 59 .9 64.1 70.5ȗ 77.6ȗ 80.7ȗ 41.6ȗ 55.7ȗ 55.7ȗ 56.1ȗ 53.8ȗ TN, N,, bbut ut B P 2.3 22.6 2. 6 2.5 - No HTN, BP 3.6ȗ 0.9ȗ 55.2ȗ 5.2 .2ȗ 0.3ȗ 1. .5ȗ 3.7ȗ 1.5ȗ 0.8ȗ 0mm mmHg Hg† >160/100mmHg - HTN and and n L LVH V † VH 221.7 1.77 21.1 21 . .1 20.4 20 0.4 330.8ȗ 30 0.88ȗ 111.7ȗ 1.7ȗ . ȗ 446.2ȗ 6.2ȗ 6.2 6.6 .66ȗ 111.1ȗ 1.11ȗ 10.9 10 .9ȗȗ 6.6ȗ 10.9ȗ 38.1ȗ † okee or TIA 113.8 3.88 15.4 15 .44 114.6 4.6 12 12.0 2.00 112.5 2.5 2.5 111.5 11 .5 14.1 Prior Stroke 7.4* 4 118.8* 8 8* 8. 8 222.1* 2 1* 2. 1* † Prior MI 114.4 4.44 115.7 5.7 15.5 5 17.2 7 17.2* 1 .2* 17 18 18.2* .2* 118.1* 18 .1** .1 7. 7.3* 3* 3* 10. 10.9* 0 9* 9 5.5* Heart Failure ailur ure re† 334.7 4.77 35.3 35 5.33 337.4 37 .44 27.8* 277.8* 8* 21.2* 21 1.2 . * 58.5 58 58.5* 8.5 .5** 117.7* 17 .7* 7* 26.3* 26.3 26 .3* 28.4* 28.4 28 . * .4 63.8* LV Systolic olicc Dysfunction Dysffunnct Dy ctio i n† 223.7 3.7 21.8 21 .8 24.1 24 15 .1* 1* 29 .5* 5* 16.1* 16 31.9 31 .9** 19 9.2** 117.2* 17 .2* 2* 15.1* 29.5* 31.9* 19.2* 46.1* † Rheumatic tic Heart Diseas Disease se 11.6 11. 1.66 2.2* 2. 2 66.7* .7* .7 1.5* 1. 33.8* .8* .8 331.5* 31 .55* 115.7* 15 .77* 3.6* 3. 6 15.3* 21.5* † Valvularr Heart Disease 221.7 1.77 224.9 24 .99 23.7 16.2* 16 .2* .2 2* 8.8* 8. 8* 110.7* 0 7* 0. 446.7* 6.7** 116.7* 6.7* 6. 7* 116.6* 6.6* 6. 6 6* 32.6* † Pacemaker 4.7 4.1 3.8 8.6* 7.9* 6.9* 1.6* 3.2* 2.6* 1.1* Congenital Heart Disease† 2.2 2.0 2.5 1.6 1.8 2.0 1.9 4.3* 1.2* 2.1* † 1.2 0.9 1.4 0.7 0.7 1.5 1.3 Recent Cardiac Surgery 3.3* 0.3* 0.4* † CHADS2 Score, mean (SD) 1.8 (1.4) 2.0* (1.4) 2.0* (1.3) 1.6* (1.3) 2.3* (1.2) 1.1* (1.1) 1.8 (1.4) 2.0* (1.5) 1.6* (1.4) 1.8 (1.3) † 3.8 3.4 3.9 2.6 2.4 History of Major Bleeding 7.9* 5.6* 1.5* 2.3* 5.7* ‡ † Lone Atrial Fibrillation 10.7 13.1* 8.2* 19.2* 4.4* 6.3* 13.0* 13.6* 17.9* 5.6* Other Concomitant Conditions Diabetes Mellitus† 21.8 24.4 20.2 18.1* 17.1* 26.7* 15.5* 29.2* 36.2* 14.0* Region
Over all
21 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
COPD† Obesity (BMI 35)† OSA† Hyperthyroidism† Pericarditis† Tuberculosis† HIV† Endomyocardial Fibrosis† Other risk factors History of Tobacco Use† Alcohol mean/week†>14/week†
11.5 7.2 3.9 3.7 0.8 1.4 0.3 0.2
16.9* 15.2* 10.1* 2.8 0.6 0.3* 0.2 0.0
17.0 3.0 1.4
20.9* 4.1*1.8
10.2 7.2 4.1 1.2* 0.8 1.1 0.0 0.2
9.8 9.0 4.0 3.8 0.5 0.2* 0.0 0.1
23.4* 12.5* 5.8* 7.0* 0.9 2.2* 0.0* 0.0
17.0 16.0 17.3 0.8*0.3* 5.6*4.4* 2.1*1.1
4.8* 2.2* 0.8* 2.2* 0.7 0.4* 0.0* 0.0
11.7 0.6* 3.5 3.3 0.4 3.9* 0.0 0.0
6.6* 1.3* 0.7* 5.4* 0.3 2.4* 0.0 0.1
6.4* 11.4* 3.3 2.6 0.3 0.2* 0.0 0.0
4.7* 6.4 1.3* 3.1 3.1* 1.8 4.0* 2.3*
7.5* 0.9*0.2*
21.6* 2.81.3
24.5* 24 24.5 .55* 11.7*0.8 1. .7*0. *0. 08
20.6* 20 20.6 .6** 00.9*0.2* 0. .9* 9 0. 9* 0 2* 2
12.6* 3.61.9
All numbers ers are percentages, except where stated. *Significantly ntly different from the rest of the world, p<0.005 † Significant nt difference among the 9 regions, p<0.001 ‡Age 60 0 year years arss wi with without thou th outt co ou conc concomitant ncom nc o it itan antt ca an cardiovascular disease (including hypertension), hypertension on)), ), ppulmonary u monary disease, hyperthyroidism ul hyperthyro roid idis id i m or recent cardiac surgery. is IQR – Interquartile Ventricular (documented BP erq rqua uart ua rtil ille range, r ngge, ra e, HTN HTN T – Hypertension, Hype Hy p rtension, LV- Left Ventricular; LVH – Leftt Ve pe V ntri tr cular Hypertrophy (d doc o um men ente nte tedd by electrocardiogram or echocardiogram); echocardiog – Blood Pressure; Chronic Obstructive Pulmonary Disease res essure r ; OSA re O A – Obstructive OS Obst Ob bs ructi tive ve Sleep Sleeep Apnea, Apn pnea ea,, COPD PD – Chr hroniic Ob bst s ru ructiv ivee Pu lmon lm o ary Di Dise seas asee
22 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Table 3. Medication prior to study entry in patients with a prior history of AF or other predisposing conditions Region
Over all
Number of patients Aspirin† Clopidogrel /ticlopidine† Dipyramidole† Warfarin† Other Vitamin itamin K antagonist† TTR (mean) ean)† Diureticss† ACE-inhibitor hibitor† ARB† cker† Beta-blocker Verapamil miil /D /Dil /Diltiazem illti tiaz a em m† † Digoxin Amiodarone ronee† ro Flecainide d † de Propafenone non one† Sotalol† Disopyramide amiide† Dofetilide de Quinidine n e† Other anti-arrythmic† Statin† Other lipid lowering† Management of Patients with HTN Medical Therapy for hypertension† Systolic BP, mean mm Hg (SD)†
15400 36.2 7.7 0.4 23.3 7.1 48.6 43.3 29.7 14.4 41.8 8.2 223.4 3.44 3. 88.7 .77 00.8 .8 22.0 .0 22.0 .00 0.1 00.0 . .0 00.1 .11 1.8 26.3 2.7
North South Western Eastern America America Europe Europe 1817 1134 1983 2542 40.4* 43.1* 33.2* 38.6* 8.1 7.8 3.6* 6.2* 0.2 0.1 0.2 0.9* 24.3 24.2 42.6* 21.1* 1.2* 9.9* 17.4* 12.4* 50.9 46.8 62.4* 56.0* 43.9 51.6* 40.3* 49.4* 31.6 42.4* 32.6* 53.6* 15.7 22.4* 16.6* 9.7* 44.2 49.9* 52.1* 49.9 49 9* 53.2* 77.5 7. 5 18.5* 5.3* 2.7* 23.1 23 .1 14.4* 14.4 14 .4* 12 12.7* .7* 7* 18.1* 18.1 18 .1* 44.7* 4. 7 7* 117.2* 7.2** 5.2* 5.2 . * 15.9* 15.9 .9* 9 1.22 0.1 3. .9** 0.0 .0** 3.9* 0.0* 2.5 11.4 1. 4 11.8 .8 4.4* 4. 4* 4* 33.9* .9* 9* 00.4* .44* 55.0* 5. 0** 33.4* .4** .4 0.11 00.0 0. 0 0.2 0.5* 5* 0.00 0. 00.0 0. 0 0.00 0. 0.2* 0. 2 00.1 .11 00.0 .00 00.0 .00 0.6* 0.6* 6 1.0 2.6 1.4 3.6* 23.5 42.2* 35.3* 39.0* 6.7* 1.2* 4.1* 1.6*
India 2536 24.1* 14.2* 0.3 14.2* 9.3* 33.7* 47.1* 14.6* 8.4* 27.7* 114.3* 4 3* 4. * 37.3* 37.3 37 . * 110.0 0.0 0 1* 0. 0.1* 00.0* .0* 00.1* 0. 1* 00.00 0. 0.00 0. 0.0 0.00 0.9* 9.4* 4.4*
China South East Asia 2023 1341 35.1 48.4* 9.0 4.3* 0.3 0.6 13.1* 31.8* 0.6* 0.7* 0. 7 7* 35.5* 36 36.0* 6.0* 0* 32.3* 33.1* 32.3 32 .33* 18.6* 13.2* 15.0 24.5* 40.1 37.1* 8.8 4.5* 21.0 2 .0 21 27.3* 27.33* 77.2 .2 66.1* 6. 1* 0.7 07 0. 0.0 . * 0.0* 22.00 2. 3. 3.9* 9** 1.22 1. 00.6* .6* .6 6* 0.0 00 0. 0.1 01 0. 00.0 0. 0 0.00 0. 0.0 0.00 0.0 0.00 2.2 1.9 17.4* 29.8* 1.9 0.2*
Middle Africa East 887 1137 38.1 27.2* 10.7* 1.1* 0.7 0.8 33.1* 15.9* 00.2* .2** .2 3.5* 42.2 42 .2 32.7* 40 40.1 .11 50.7* 32.1 24.1* 19.8* 6.8* 44.0 21.7* 6.2 2.0* 21.9 21. 1.99 34.5* 33.5* .5* 5* 3.3* 00.22 0. 0.2 00.1* .1* 0.1* 00.7* 0. 7** 0.4* 0.0 00 0. 0.0 0.0 0.0 0.0 0.00 0.0 1.4 0.3* 30.0 6.2* 1.0* 0.4*
92.9
96.3ȗ
97.2ȗ
95.4*
89.7ȗ
95.5ȗ
91.0
88.9ȗ
94.0
89.2ȗ
138.1 (25.4)
136.7 (25.8)
136.3 (27.0)
138.4 (25.3)
140.5 (22.7)ȗ
133.4 (22.2)ȗ
140.0 (23.2)
136.8 (29.5)
138.1 (28.1)
142.2 (29.0)ȗ
23 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Diastolic BP, mean mm Hg (SD)† Management of Patients with HF and/or LV dysfunction ACE Inhibitor or ARB† Beta-blocker at baseline†
82.4 (15.9)
79.8 (17.1)ȗ
82.1 (16.7)
82.5 (17.1)
84.5 (12.8)ȗ
82.6 (12.2)
83.0 (15.7)
77.9 (18.9)ȗ
80.5 (17.6)
87.2 (16.9)ȗ
51.9 45.6
59.3* 63.0*
67.5* 48.8
61.4* 63.9*
63.1* 54.0*
31.6* 30.4*
36.3* 39.9*
46.9 43.3
60.5* 56.2*
61.7* 19.9*
All numbers are percentages, except where stated. HTN – Hypertension, BP – Blood Pressure, LVH – Left Ventricular Hypertrophy, ACE – Angiotensin Converting Enzyme, ARB – Angiotensin Receptor Blocker, TTR – Time in therapeutic range *Significantly different from the rest of the world, p<0.005 ȘSignificant nt difference among the 9 regions, p<0.001
24 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
DOI: 10.1161/CIRCULATIONAHA.113.005451
Figure Legends:
Figure 1. Proportion of patients with rheumatic heart disease. *Significantly different from the rest of the world, p<0.005.
Figure 2. Proportions of patients with a prior history of atrial fibrillation who were receiving an oral anticoagulant at presentation to the emergency department.
Figure 3. INR control based on the three most recent values prior to presentation to the emergency department.
25 Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
* * *
* Gl Global G average 11.6% 1 11
Figure 1
Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
Rheum Rh Rheumatic Glob Gl o a average 46.4% Global Non-rheumatic, NonNo n-rr CHADS2 2 CHAD Global Globa average 34.4%
Figure 2
Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
Global INR >3.0 = 14.1%
36 54
67 44
35
46 59
39
41 Global INR 2.0-3.0 2.0-3 = 50.3% Global Glob Gl obal al INR INR < <2.0 2.0 = 35.5%
Figure 3
Downloaded from http://circ.ahajournals.org/ by guest on January 27, 2014
SUPPLEMENTAL MATERIAL
North America
South America
West Europe
East Europe
India
China
SE Asia
Middle East
Africa
Supplemental Table 1. Baseline Cardiovascular Risk Factors for Atrial Fibrillation after Excluding Patients with Cardiovascular Surgery, Congenital Heart Disease, Rheumatic Heart Disease, Tuberculosis, Pericarditis, Endomyocardial Fibrosis, Chagas Disease and HIV
Number of patients Age, mean (SD) years† Male†
1709
981
1904
2268
1628
1584
1229
724
807
70.4 ± 13.2* 58.7*
69.4 ± 12.6* 57.7
69.7 ± 12.0* 62.0*
69.4 ± 10.9* 50.5*
62.8± 14.6* 54.2
70.2±1 2.5* 49.4*
69.8±1 3.2* 55.9
60.2± 15.5* 59.4
64.5±1 3.7* 49.9*
Prior MI†
17.7
16.6
18.4*
17.9
20.0*
8.7*
10.7*
19.9*
7.2*
Left Ventricular Dysfunction† Heart Failure †
15.0*
28.3*
16.1*
31.6*
26.9*
17.0*
16.9*
22.8*
49.3*
27.2*
34.1
20.9*
56.3*
18.8*
30.6
25.0*
26.5*
61.1*
Hypertension†
70.9*
79.9*
60.5*
82.7*
55.3*
62.1*
65.1
60.9*
69.0
Valvular Disease†
14.4
19.1*
7.8*
7.9*
28.9*
4.6*
13.8
10.2
14.5
Diabetes Mellitus†
24.5
19.2*
17.4*
26.3*
24.9
16.6*
29.5*
39.0*
17.8*
Region
All numbers are percentages, except age. MI – Myocardial Infarction, SE Asia – South-East Asia *Significantly different from the rest of the world, p<0.005 †Significant difference among the 9 regions, p<0.001
Appendix. Investigators in the RE-LY AF Registry Argentina:A. Caccavo, F. Risso, A. Sanchez; Australia:Dr. B. Singh; Austria: Dr. F. Freihoff; Brazil: C. A. K. Abunader, J. F. S. Kerr, P. E. Leães, H. J. R. Lima, A. L. F. Menezes, L. M. Nigro, D. B. Precoma, L. E. Ritt, F. R. dos Santos, W. F. Saporito, A. C. S. Sobral, F. S. Tallo, L. A. Vidal; Bulgaria: N. Gocheva, D. Raev; Cameroon: M. Ntep-Gweth, A. D. Tamdja; Canada: D. Cleveland, P. Dorian, J.Healey, C. Lai, M. Mantle, C. Morillo, G. O'Hara, R. Parkash; Chile: F. Lanas, C. Marcelo, P. Varleta; China: X. Bai, J. Y. Han, Q. He, X. Hui, C. Li, J. Li, S. Liu, J. Lu, H. S. Tang, S. Wang, Y. Yanmin, P. Yu, Z. Zan, H. Zeng, F. Zhang, F. Zhang, H. Zhang, Q. Zhang, L. Zhao, Z. X. Zhou; Colombia: L. F. Pava, F. R. D. Quiros; Czech Republic: J. Bednar, H. Grunfeldova, O. Hejhal, J. Jakabcin, Z. Jelinek, J. Kral, A. Mandovec, D. Vaclav; Denmark: A. Brandes; Ecuador: R. Vicuna; Egypt: I. Shawky, A. F. Tamara; Germany: K. Appel, J. Harenberg, U. Hoffmann, T. Horacek; Hungary: L. Csiba, K. Keltai, E. Kis; India: R.K. Agarwal, V. Arora, R. Babu, A. Bharani, D. Banker, S. Diwedi, J.B. Gupta, J. Hiremath, R. K. P. Jain, J. Joseph, S. Kumar, P. Lavhe, A. Naik, R.B. Panwar, T. Patel, B. Pinto, J.P.S. Sawhney, S. Shah, A. Srinivas, S. K. Trivedi, K. Varghese, S. Verma; Iran: M.R. M. Hasani; Italy: D. Coen, A. Salvioni; Japan: E. Watanabe; Kenya: G. Yonga; Korea: S. H. Hu, C. Jeong-Gwan, J. S. Kim, N. H. Kim, M. Y. Lee, K. Y. Nyun, T. H. Rho; Latvia: A. Apinis, G. Dormidontova, I. Zakke; Mozambique: A. Demasceno, A. O. H. Mocumbi; Netherlands: J.V.M. van Eck, I. van Gelder; Nigeria: A. Akinyemi, V. Ansa, S. S. Danbauchi, E. Emmanuel, K. M. Karaye, O. S. Ogah, D. Ojji, M. U. Sani; Poland: P. Miekus; Russia: S. S. Yakushin; Saudi Arabia: B. Al Ghamdi; Senegal: S. Abdou; Singapore: S. H. Lim, S. O. B. Suat; Slovakia: J. Strbova, D. Vinanska; South Africa: A. K. M. N. Alam, P. Commerford, K. Sliwa; Spain: G. T. Gusi; Sudan: A. Suliman; Sweden: J. Herlitz, Z. Hijazi, L. Malmqvist, P. J. Svensson; Tanzania: M. Janabi; Thailand: S. Tanomsup; Turkey: B. Yavuz; United Arab Emirates: W. Almahmeed, G. A. Radaidah, A. H. Yusufali; Uganda: M. C. Kiiza; Ukraine: O. Grishyna, O. Onyshchenko; United Kingdom: A. Moriarty, M. Pye, R. Sheahan; United States: V. Duthinh, E. Gillespie, I. Haque, D. Huckins, R. Khant, W. N. Leimbach Jr., C. McPherson, A. Murphy, A. Rasinghani, A. Storrow, M. Williams; Venezuela: I. Mendoza; Zambia: F. Goma.
2